

Persistent Vascular Complications in Long COVID: The Role of ACE2 Deactivation, Microclots, and Uniform Fibrosis
- PMID: 39051242
- PMCID: PMC11270324
- DOI: 10.3390/idr16040042
Persistent Vascular Complications in Long COVID: The Role of ACE2 Deactivation, Microclots, and Uniform Fibrosis
Abstract
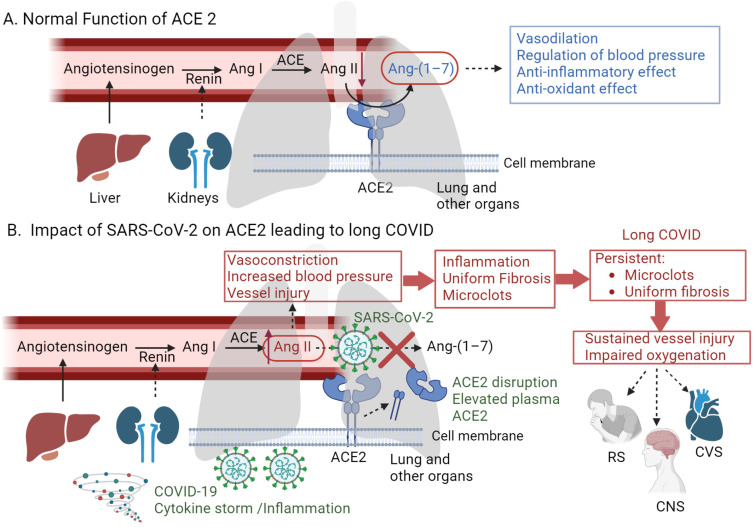
Angiotensin-converting enzyme 2 (ACE2), a key regulator in vasoregulation and the renin-angiotensin system, is hypothesized to be downregulated in patients with COVID-19, leading to a cascade of cardiovascular complications. This deactivation potentially results in increased blood pressure and vessel injury, contributing to the formation and persistence of microclots in the circulation. Herein, we propose a hypothesis regarding the prolonged vascular complications observed in long COVID, focusing on the role of ACE2 deactivation and/or shedding, the persistence of microclots, and the unique pattern of fibrosis induced by severe acute respiratory syndrome-coronavirus-2 (SARS-CoV-2). Furthermore, we propose that the distinctive, uniform fibrosis associated with COVID-19, which is challenging to detect through conventional X-ray imaging, exacerbates vascular injury and impairs oxygenation. The persistence of these microclots and the unique fibrosis pattern are suggested as key factors in the extended duration of vascular complications post-COVID-19 infection, regardless of the initial disease severity. Moreover, plasma ACE2 activity has the potential to serve as prognostic or diagnostic biomarkers for monitoring disease severity and managing long COVID symptoms. Elucidating the role of ACE2 deactivation and the consequent events is vital for understanding the long-term effects of COVID-19. The experimental verification of this hypothesis through in vitro studies, clinical longitudinal studies, and advanced imaging techniques could yield significant insights into the pathophysiological mechanisms underlying long COVID, thereby improving the management of patients, particularly those with cardiovascular complications.
Keywords: ACE2; RAS; fibrosis; long COVID; microclots; severe acute respiratory syndrome-coronavirus-2; vasoregulation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Testing the efficacy and safety of BIO101, for the prevention of respiratory deterioration, in patients with COVID-19 pneumonia (COVA study): a structured summary of a study protocol for a randomised controlled trial.Trials. 2021 Jan 11;22(1):42. doi: 10.1186/s13063-020-04998-5. Trials. 2021. PMID: 33430924 Free PMC article.
-
Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2.Circ Res. 2020 May 8;126(10):1456-1474. doi: 10.1161/CIRCRESAHA.120.317015. Epub 2020 Apr 8. Circ Res. 2020. PMID: 32264791 Free PMC article. Review.
-
Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19).J Pathol. 2020 Jul;251(3):228-248. doi: 10.1002/path.5471. Epub 2020 Jun 10. J Pathol. 2020. PMID: 32418199 Free PMC article. Review.
-
Disequilibrium between the classic renin-angiotensin system and its opposing arm in SARS-CoV-2-related lung injury.Am J Physiol Lung Cell Mol Physiol. 2020 Aug 1;319(2):L325-L336. doi: 10.1152/ajplung.00189.2020. Epub 2020 Jul 8. Am J Physiol Lung Cell Mol Physiol. 2020. PMID: 32639866 Free PMC article. Review.
-
Effects of SARS-CoV-2 on Cardiovascular System: The Dual Role of Angiotensin-Converting Enzyme 2 (ACE2) as the Virus Receptor and Homeostasis Regulator-Review.Int J Mol Sci. 2021 Apr 26;22(9):4526. doi: 10.3390/ijms22094526. Int J Mol Sci. 2021. PMID: 33926110 Free PMC article. Review.
References
-
- Stawicki S.P., Jeanmonod R., Miller A.C., Paladino L., Gaieski D.F., Yaffee A.Q., De Wulf A., Grover J., Papadimos T.J., Bloem C., et al. The 2019–2020 novel coronavirus (severe acute respiratory syndrome coronavirus 2) pandemic: A joint american college of academic international medicine-world academic council of emergency medicine multidisciplinary COVID-19 working group consensus paper. J. Glob. Infect. Dis. 2020;12:47–93. doi: 10.4103/jgid.jgid_86_20. - DOI - PMC - PubMed
-
- Silva Andrade B., Siqueira S., de Assis Soares W.R., de Souza Rangel F., Santos N.O., dos Santos Freitas A., Ribeiro da Silveira P., Tiwari S., Alzahrani K.J., Góes-Neto A., et al. Long-COVID and post-COVID health complications: An up-to-date review on clinical conditions and their possible molecular mechanisms. Viruses. 2021;13:700. doi: 10.3390/v13040700. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
