

Ronapreve (REGN-CoV; casirivimab and imdevimab) reduces the viral burden and alters the pulmonary response to the SARS-CoV-2 Delta variant (B.1.617.2) in K18-hACE2 mice using an experimental design reflective of a treatment use case
- PMID: 39012120
- PMCID: PMC11302283
- DOI: 10.1128/spectrum.03916-23
Ronapreve (REGN-CoV; casirivimab and imdevimab) reduces the viral burden and alters the pulmonary response to the SARS-CoV-2 Delta variant (B.1.617.2) in K18-hACE2 mice using an experimental design reflective of a treatment use case
Abstract
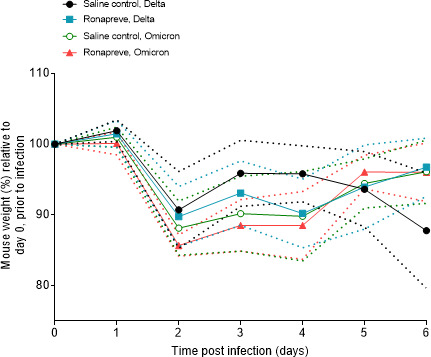
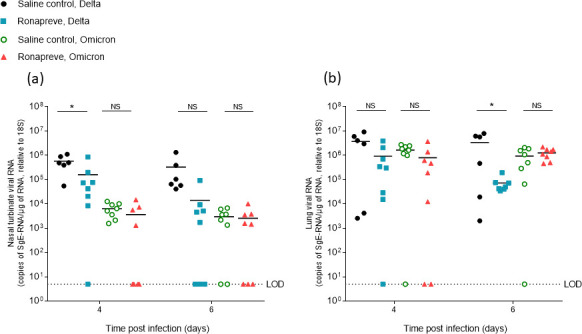
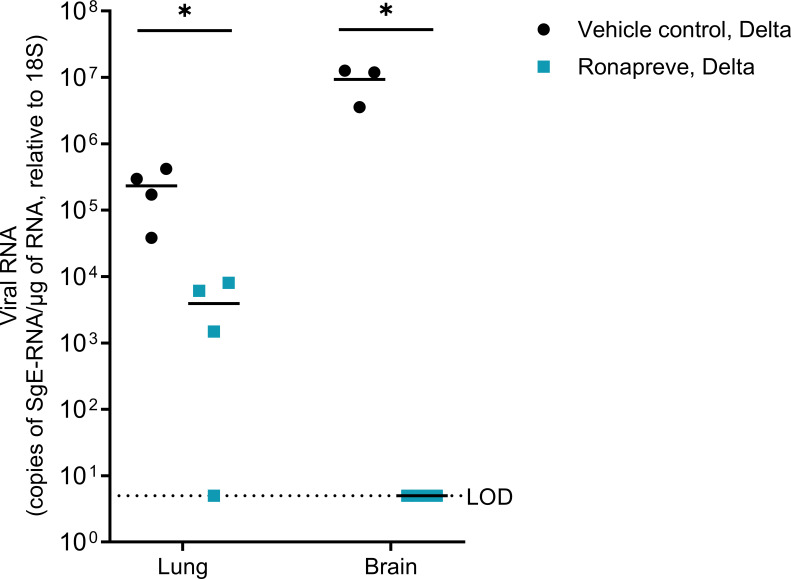
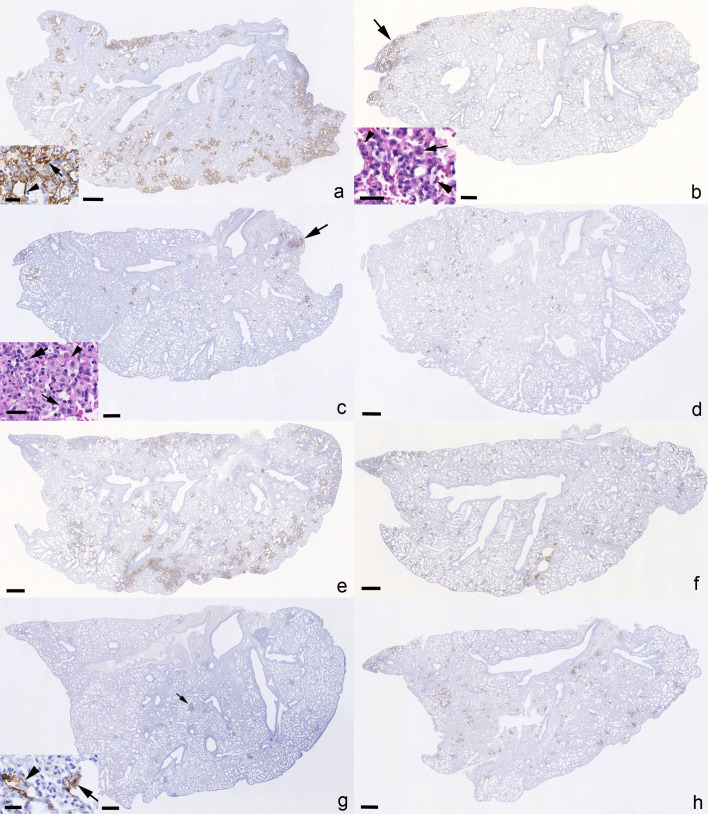
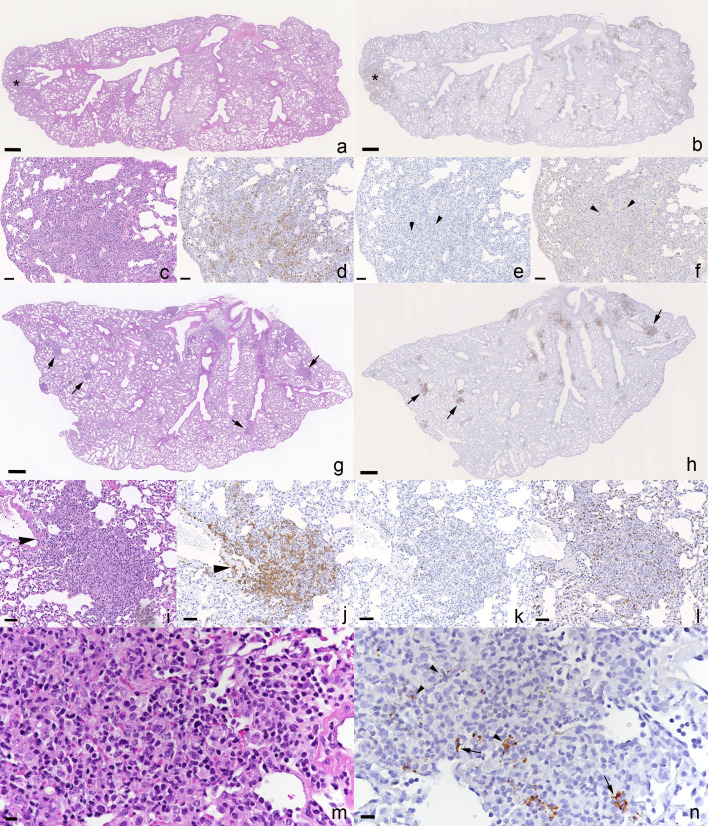
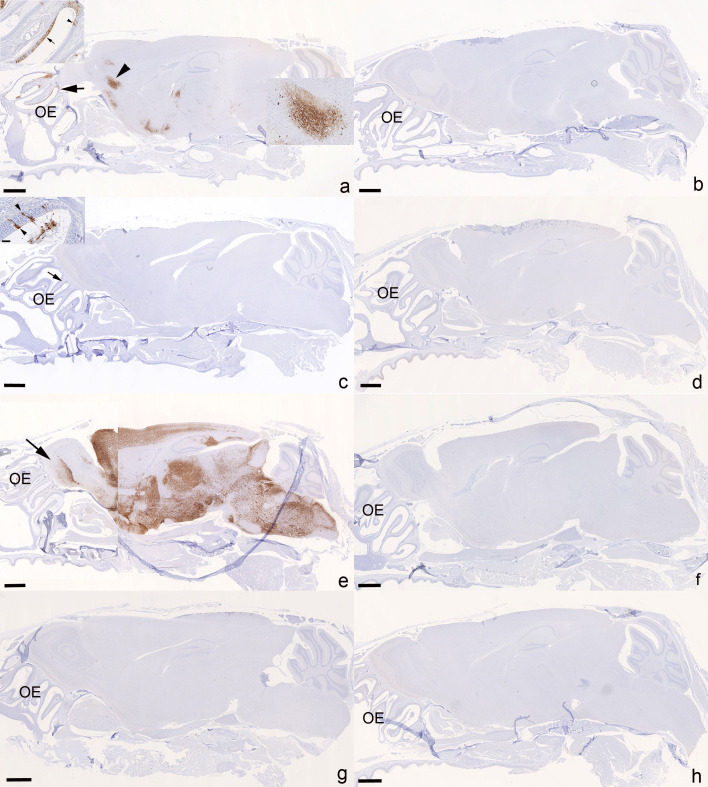
With some exceptions, global policymakers have recommended against the use of existing monoclonal antibodies in COVID-19 due to loss of neutralization of newer variants. The purpose of this study was to investigate the impact of Ronapreve on compartmental viral replication using paradigms for susceptible and insusceptible variants. Virological efficacy and impact on pathogenicity was assessed in K18-hACE2 mice inoculated with either the Delta or BA.1 Omicron variants. Ronapreve reduced sub-genomic viral RNA levels in lung and nasal turbinate, 4 and 6 days post-infection, for the Delta variant but not the Omicron variant. It also blocked brain infection, which is seen with high frequency in K18-hACE2 mice after Delta variant infection. At day 6, the inflammatory response to lung infection with the Delta variant was altered to a multifocal granulomatous inflammation in which the virus appeared to be confined. The current study provides evidence of an altered tissue response to SARS-CoV-2 after treatment with a monoclonal antibody combination that retains neutralization activity. These data demonstrate that experimental designs that reflect treatment use cases are achievable in animal models for monoclonal antibodies. Extreme caution should be taken when interpreting prophylactic experimental designs that may not be representative of treatment.IMPORTANCEFollowing the emergence of the SARS-CoV-2 Omicron variant, the WHO recommended against the use of Ronapreve in its COVID-19 treatment guidelines due to a lack of efficacy based on current pharmacokinetic-pharmacodynamic understanding. However, the continued use of Ronapreve, specifically in vulnerable patients, was advocated by some based on in vitro neutralization data. Here, the virological efficacy of Ronapreve was demonstrated in both the lung and brain compartments using Delta as a paradigm for a susceptible variant. Conversely, a lack of virological efficacy was demonstrated for the Omicron variant. Comparable concentrations of both monoclonal antibodies were observed in the plasma of Delta- and Omicron-infected mice. This study made use of a reliable murine model for SARS-CoV-2 infection, an experimental design reflective of treatment, and demonstrated the utility of this approach when assessing the effectiveness of monoclonal antibodies.
Keywords: SARS-CoV-2; mAb; preclinical PK/PD.
Conflict of interest statement
A.O. and S.R. are directors of Tandem Nano Ltd. and co-inventors of patents relating to drug delivery. A.O. has been a co-investigator on funding received by the University of Liverpool from ViiV Healthcare and Gilead Sciences unrelated to COVID-19 in the past 3 years. A.O. has received personal fees from Gilead and Assembly Biosciences in the past 3 years unrelated to COVID-19. A.O. was a member of the Trial Management Group for the AGILE phase I/II platform trial until January 2023 and AGILE received funding from Ridgeback and GSK in the past 3 years for which A.O. was not a co-investigator. S.R. has received research funding from ViiV and AstraZeneca, and consultancy from Gilead not related to the current paper. No other conflicts are declared by the authors.
Figures
Update of
-
Ronapreve (REGN-CoV; casirivimab and imdevimab) reduces the viral burden and alters the pulmonary response to the SARS-CoV-2 Delta variant (B.1.617.2) in K18-hACE2 mice using an experimental design reflective of a treatment use case.bioRxiv [Preprint]. 2023 Mar 9:2022.01.23.477397. doi: 10.1101/2022.01.23.477397. bioRxiv. 2023. Update in: Microbiol Spectr. 2024 Aug 6;12(8):e0391623. doi: 10.1128/spectrum.03916-23 PMID: 35118468 Free PMC article. Updated. Preprint.
Similar articles
-
Ronapreve (REGN-CoV; casirivimab and imdevimab) reduces the viral burden and alters the pulmonary response to the SARS-CoV-2 Delta variant (B.1.617.2) in K18-hACE2 mice using an experimental design reflective of a treatment use case.bioRxiv [Preprint]. 2023 Mar 9:2022.01.23.477397. doi: 10.1101/2022.01.23.477397. bioRxiv. 2023. Update in: Microbiol Spectr. 2024 Aug 6;12(8):e0391623. doi: 10.1128/spectrum.03916-23 PMID: 35118468 Free PMC article. Updated. Preprint.
-
The lethal K18-hACE2 knock-in mouse model mimicking the severe pneumonia of COVID-19 is practicable for antiviral development.Emerg Microbes Infect. 2024 Dec;13(1):2353302. doi: 10.1080/22221751.2024.2353302. Epub 2024 May 26. Emerg Microbes Infect. 2024. PMID: 38753462 Free PMC article.
-
Human convalescent plasma protects K18-hACE2 mice against severe respiratory disease.J Gen Virol. 2021 May;102(5):001599. doi: 10.1099/jgv.0.001599. J Gen Virol. 2021. PMID: 33961540 Free PMC article.
-
SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19.Cochrane Database Syst Rev. 2022 Jun 17;6(6):CD014945. doi: 10.1002/14651858.CD014945.pub2. Cochrane Database Syst Rev. 2022. PMID: 35713300 Free PMC article. Review.
-
Evolution of the SARS-CoV-2 omicron variants BA.1 to BA.5: Implications for immune escape and transmission.Rev Med Virol. 2022 Sep;32(5):e2381. doi: 10.1002/rmv.2381. Epub 2022 Jul 20. Rev Med Virol. 2022. PMID: 35856385 Free PMC article. Review.
Cited by
-
Sensitivity to Vaccines, Therapeutic Antibodies, and Viral Entry Inhibitors and Advances To Counter the SARS-CoV-2 Omicron Variant.Clin Microbiol Rev. 2022 Sep 21;35(3):e0001422. doi: 10.1128/cmr.00014-22. Epub 2022 Jun 6. Clin Microbiol Rev. 2022. PMID: 35862736 Free PMC article. Review.
-
Animal efficacy study of a plant extract complex (BEN815) as a potential treatment for COVID-19.PLoS One. 2023 Sep 14;18(9):e0291537. doi: 10.1371/journal.pone.0291537. eCollection 2023. PLoS One. 2023. PMID: 37708114 Free PMC article.
References
-
- WHO . 2022. Vaccine equity. https://wwwwhoint/campaigns/vaccine-equity.
-
- Horby P. 2021. Antiviral drug resistance and the use of directly acting antiviral drugs (DAAs) for COVID-19. New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) - https://wwwgovuk/government/publications/nervtag-antiviral-drug-resistan....
-
- Simões EAF, Forleo-Neto E, Geba GP, Kamal M, Yang F, Cicirello H, Houghton MR, Rideman R, Zhao Q, Benvin SL, Hawes A, Fuller ED, Wloga E, Pizarro JMN, Munoz FM, Rush SA, McLellan JS, Lipsich L, Stahl N, Yancopoulos GD, Weinreich DM, Kyratsous CA, Sivapalasingam S. 2021. Suptavumab for the prevention of medically attended respiratory syncytial virus infection in preterm infants. Clin Infect Dis 73:e4400–e4408. doi:10.1093/cid/ciaa951 - DOI - PMC - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
- R01 AI134091/AI/NIAID NIH HHS/United States
- LONGEVITY/Unitaid
- EP/R024804/1, EP/S012265/1/UKRI | Engineering and Physical Sciences Research Council (EPSRC)
- R24 AI118397/AI/NIAID NIH HHS/United States
- 101057553/European Union & Horizon Europe research and innovation program
- TS/V012967/1/UKRI | Innovate UK
- 22.00094/Swiss State Secretariat for Education, Research and Innovation (SERI)
- 222489/Z/21/Z/Wellcome Trust (WT)
- WT_/Wellcome Trust/United Kingdom
- IZSEZ0, 213289/Swiss National Science Foundation (SNSF)
- R01AI134091, R24AI118397/HHS | National Institutes of Health (NIH)
- BB/R00904X/1, BB/R018863/1, BB/N022505/1/UKRI | Biotechnology and Biological Sciences Research Council (BBSRC)
- MR/W005611/1, MR/R010145/1/UKRI | Medical Research Council (MRC)
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
