

The Efficacy of Letrozole Co-Treatment in an Antagonist Protocol for Women with Polycystic Ovary Syndrome Undergoing IVF: A Retrospective Study
- PMID: 39006189
- PMCID: PMC11244072
- DOI: 10.2147/DDDT.S458608
The Efficacy of Letrozole Co-Treatment in an Antagonist Protocol for Women with Polycystic Ovary Syndrome Undergoing IVF: A Retrospective Study
Abstract
Objective: Our objective was to investigate the efficacy of letrozole co-treatment in an antagonist protocol for infertile women with polycystic ovary syndrome (PCOS).
Patients and methods: This retrospective cohort study included infertile women with PCOS undergoing IVF/ICSI with and without letrozole co-treatment in an antagonist protocol from 2007-2021 at Shanghai Ninth People's Hospital (Shanghai, China). A total of 1559 participants were enrolled, with 1227 women in the antagonist group and 332 women in the letrozole co-treatment group. Propensity score-based patient-matching model was conducted to balance covariates between the groups. The primary outcome was the number of retrieved oocytes, with secondary outcomes including endocrine parameters, ovarian stimulation outcomes, pregnancy outcomes, and obstetrical and neonatal complications.
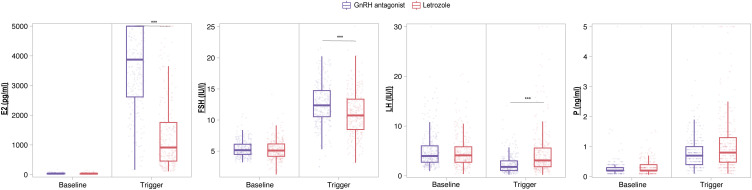
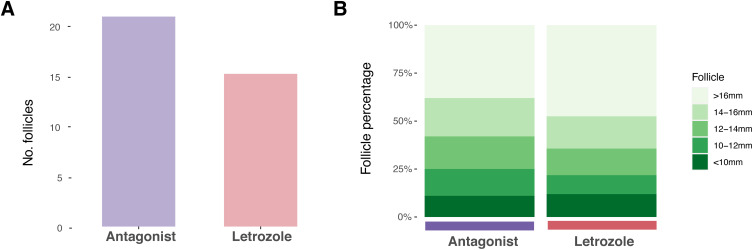
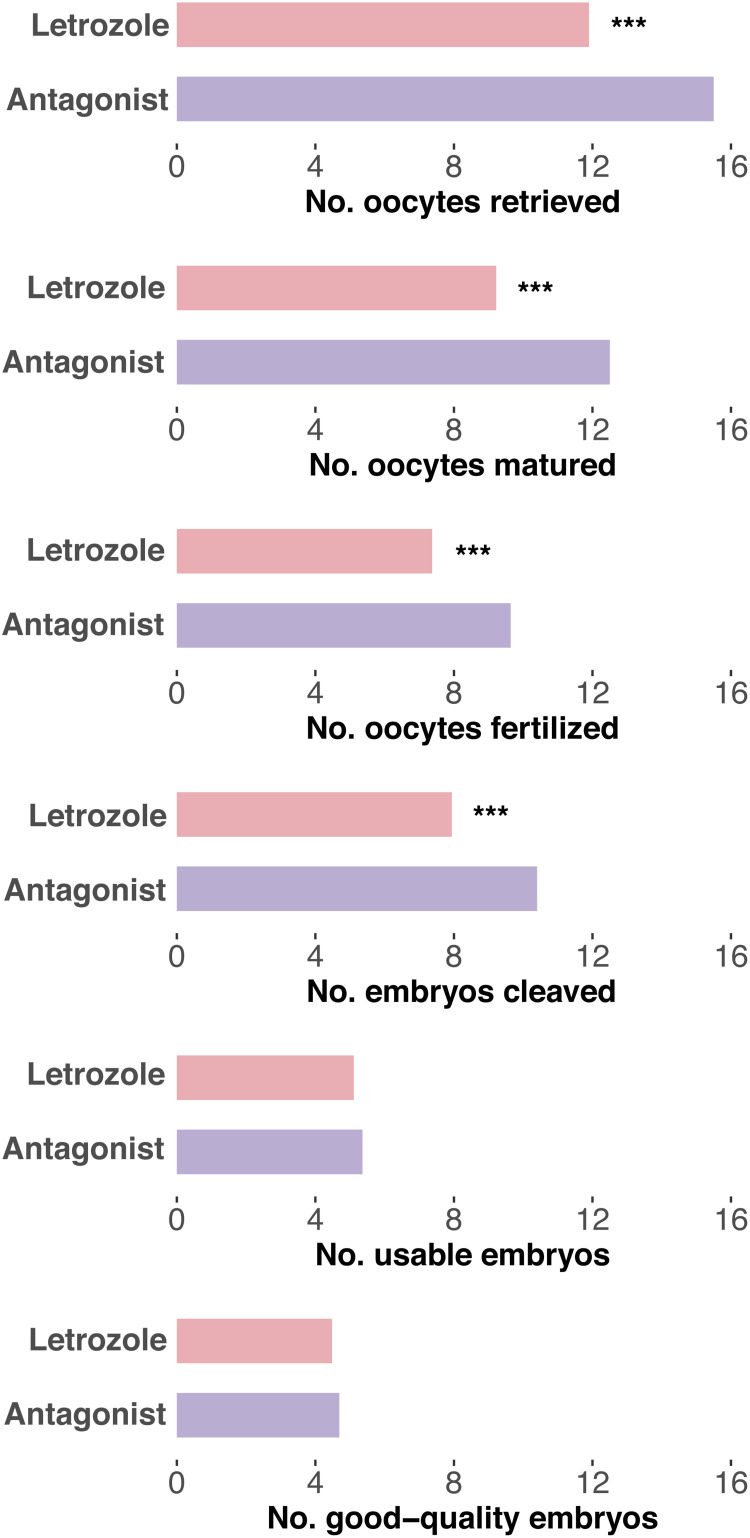
Results: Letrozole co-treatment induced significant changes in hormonal regulation, increased the percentage of large follicles, and resulted in fewer retrieved oocytes (P < 0.05). However, there was no negative impact on the number of usable embryos or good-quality embryos (P > 0.05). The live birth rates following fresh embryo transfer were comparable between the letrozole and control groups (single embryo transfer: 28.9% vs 29.7%, P > 0.05; double embryo transfer: 37.3% vs 45.6%, P > 0.05). Additionally, there were no significant differences between the two groups in the live birth rate per patient after frozen embryo transfer and the cumulative live birth rate (P > 0.05). No significant differences in obstetrical and neonatal complications were observed between the groups (P > 0.05).
Conclusion: The addition of letrozole to the antagonist protocol for women with PCOS undergoing IVF induces a higher percentage of large follicles during oocyte retrieval, while reducing the overall number of retrieved oocytes. Moreover, the use of letrozole demonstrates comparable clinical outcomes following embryo transfers. These findings highlight the potential application of letrozole in an antagonist protocol for women with PCOS.
Keywords: antagonist protocol; follicle; in vitro fertilization; letrozole; polycystic ovary syndrome.
© 2024 Lin et al.
Conflict of interest statement
The authors declare no conflicts of interest in this work.
Figures
Similar articles
-
Letrozole co-treatment in an antagonist protocol for overweight women undergoing IVF treatment: a retrospective study.BMC Pregnancy Childbirth. 2024 Sep 10;24(1):592. doi: 10.1186/s12884-024-06795-3. BMC Pregnancy Childbirth. 2024. PMID: 39256667 Free PMC article.
-
Impact of letrozole co-treatment during ovarian stimulation on oocyte yield, embryo development, and live birth rate in women with normal ovarian reserve: secondary outcomes from the RIOT trial.Hum Reprod. 2023 Nov 2;38(11):2154-2165. doi: 10.1093/humrep/dead182. Hum Reprod. 2023. PMID: 37699851 Clinical Trial.
-
Impact of letrozole co-treatment in an antagonist protocol for IVF/ICSI: a retrospective study.Reprod Biol Endocrinol. 2024 Oct 16;22(1):126. doi: 10.1186/s12958-024-01297-5. Reprod Biol Endocrinol. 2024. PMID: 39415184 Free PMC article.
-
Aromatase inhibitors (letrozole) for ovulation induction in infertile women with polycystic ovary syndrome.Cochrane Database Syst Rev. 2022 Sep 27;9(9):CD010287. doi: 10.1002/14651858.CD010287.pub4. Cochrane Database Syst Rev. 2022. PMID: 36165742 Free PMC article. Review.
-
The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance.Hum Reprod Update. 2016 Nov;22(6):687-708. doi: 10.1093/humupd/dmw025. Epub 2016 Aug 10. Hum Reprod Update. 2016. PMID: 27511809 Review.
Cited by
-
Letrozole co-treatment in an antagonist protocol for overweight women undergoing IVF treatment: a retrospective study.BMC Pregnancy Childbirth. 2024 Sep 10;24(1):592. doi: 10.1186/s12884-024-06795-3. BMC Pregnancy Childbirth. 2024. PMID: 39256667 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
