

Association between different obesity patterns and the risk of NAFLD detected by transient elastography: a cross-sectional study
- PMID: 38987694
- PMCID: PMC11238456
- DOI: 10.1186/s12876-024-03303-x
Association between different obesity patterns and the risk of NAFLD detected by transient elastography: a cross-sectional study
Abstract
Background: Obesity has become a major global public health challenge. Studies examining the associations between different obesity patterns and the risk of nonalcoholic fatty liver disease (NAFLD) are limited. This study aimed to investigate the relationships between different obesity patterns and the risk of NAFLD in a large male population in the US.
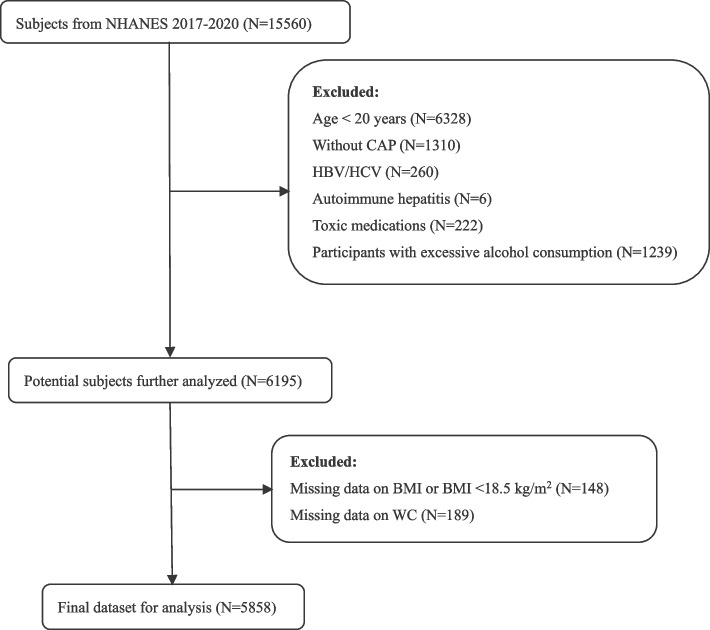
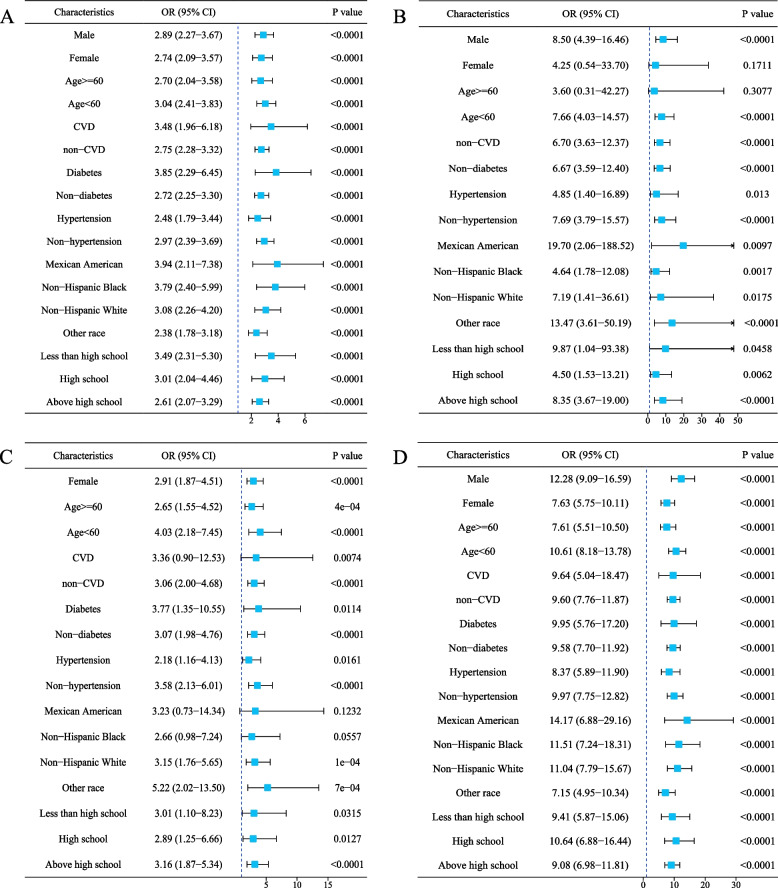
Methods: Data from the 2017 to March 2020 National Health and Nutrition Examination Survey (NHANES) were utilized. Liver steatosis and fibrosis were assessed with FibroScan using the controlled attenuation parameter (CAP) and liver stiffness measurements (LSM). Steatosis was identified with a CAP value of 248 dB/m or higher. Abdominal obesity was defined by a waist circumference (WC) of 102 cm or more for males and 88 cm or more for females. Overweight was defined as a body mass index (BMI) of 24.0 kg/m2 and above. General obesity was identified with a BMI of 28.0 kg/m2 or higher. Obesity status was categorized into four types: overweight, general obesity, abdominal obesity, and combined obesity. Multivariate logistic regression, adjusting for potential confounders, was used to examine the link between obesity patterns and NAFLD risk. Subgroup analysis further explored these associations.
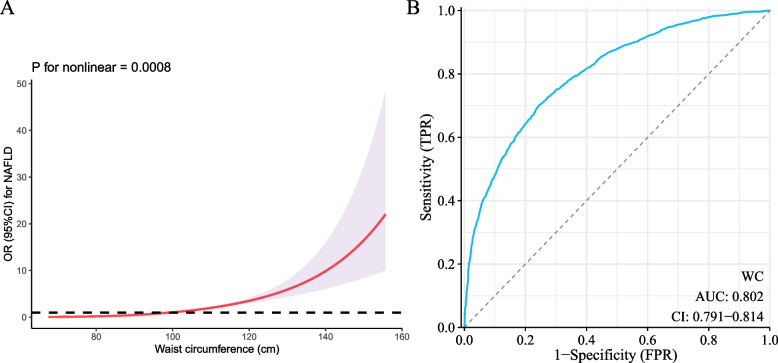
Results: A total of 5,858 adults were included. After multivariable adjustment, compared to the normal weight group, the odds ratios (ORs) [95% confidence interval (CI)] for NAFLD in individuals with overweight, general obesity, abdominal obesity, and combined obesity were 6.90 [3.74-12.70], 2.84 [2.38-3.39], 3.02 [2.02-4.51], and 9.53 [7.79-11.64], respectively. Subgroup analysis showed the effect of different obesity patterns on NAFLD risk was stable among individuals with different clinical conditions. In the fully adjusted multivariate logistic regression model, WC was positively associated with NAFLD risk (OR: 1.48; 95% CI: 1.42-1.53; P < 0.001). WC also demonstrated strong discriminatory ability for NAFLD in Receiver Operating Characteristic (ROC) analysis, achieving an Area Under the Curve (AUC) of 0.802.
Conclusions: Different patterns of obesity are risk factors for NAFLD. An increase in WC significantly increased NAFLD risk. More attention should be paid to preventing different patterns of obesity among adults.
Keywords: Cross-sectional; Hepatic fibrosis; NAFLD; Obesity patterns; Transient elastography.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Triglyceride Glucose Index and Related Parameters (Triglyceride Glucose-Body Mass Index and Triglyceride Glucose-Waist Circumference) Identify Nonalcoholic Fatty Liver and Liver Fibrosis in Individuals with Overweight/Obesity.Metab Syndr Relat Disord. 2021 Apr;19(3):167-173. doi: 10.1089/met.2020.0109. Epub 2020 Dec 1. Metab Syndr Relat Disord. 2021. PMID: 33259744
-
Triglyceride glucose-waist circumference: the optimum index to screen nonalcoholic fatty liver disease in non-obese adults.BMC Gastroenterol. 2023 Nov 2;23(1):376. doi: 10.1186/s12876-023-03007-8. BMC Gastroenterol. 2023. PMID: 37919650 Free PMC article.
-
Prevalence and factors associated with NAFLD detected by vibration controlled transient elastography among US adults: Results from NHANES 2017-2018.PLoS One. 2021 Jun 3;16(6):e0252164. doi: 10.1371/journal.pone.0252164. eCollection 2021. PLoS One. 2021. PMID: 34081733 Free PMC article.
-
Association between Sarcopenic Obesity and Nonalcoholic Fatty Liver Disease and Fibrosis detected by Fibroscan.J Gastrointestin Liver Dis. 2021 Jun 18;30(2):227-232. doi: 10.15403/jgld-3323. J Gastrointestin Liver Dis. 2021. PMID: 33951121
-
Association of different obesity patterns with hypertension in US male adults: a cross-sectional study.Sci Rep. 2023 Jun 29;13(1):10551. doi: 10.1038/s41598-023-37302-x. Sci Rep. 2023. PMID: 37386040 Free PMC article.
References
-
- Festi D, Colecchia A, Sacco T, Bondi M, Roda E, Marchesini G. Hepatic steatosis in obese patients: clinical aspects and prognostic significance. Obesity reviews : an official journal of the International Association for the Study of Obesity. 2004;5(1):27–42. doi: 10.1111/j.1467-789X.2004.00126.x. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
