

Deleterious Anti-Inflammatory Macrophage Recruitment in Early Post-Infarction Phase: Unraveling the IL-6/MCP-1/STAT3 Axis
- PMID: 38984050
- PMCID: PMC11228110
- DOI: 10.1016/j.jacbts.2024.01.019
Deleterious Anti-Inflammatory Macrophage Recruitment in Early Post-Infarction Phase: Unraveling the IL-6/MCP-1/STAT3 Axis
Abstract
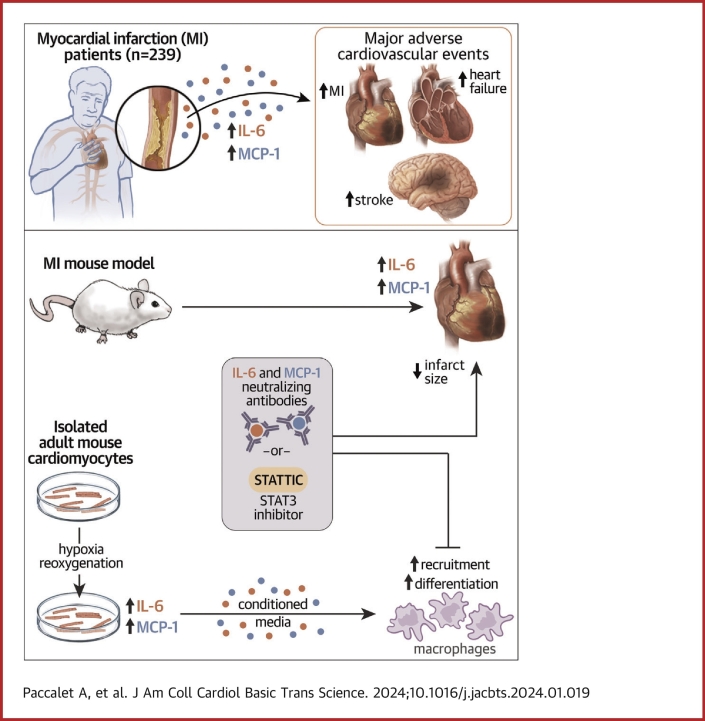
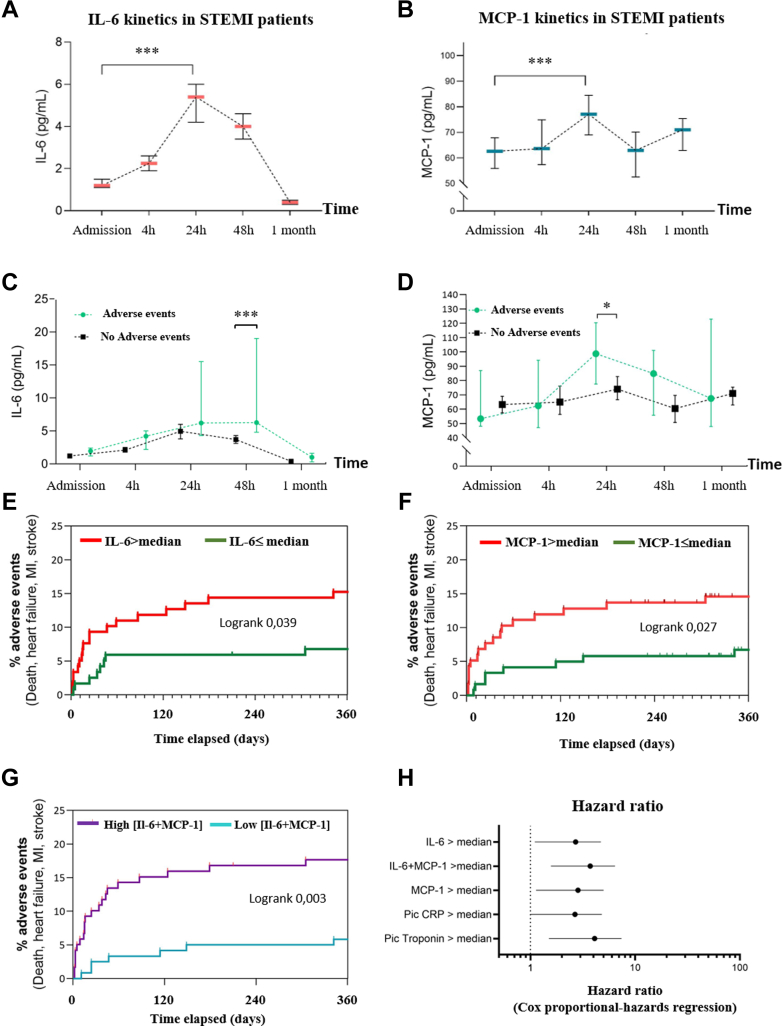
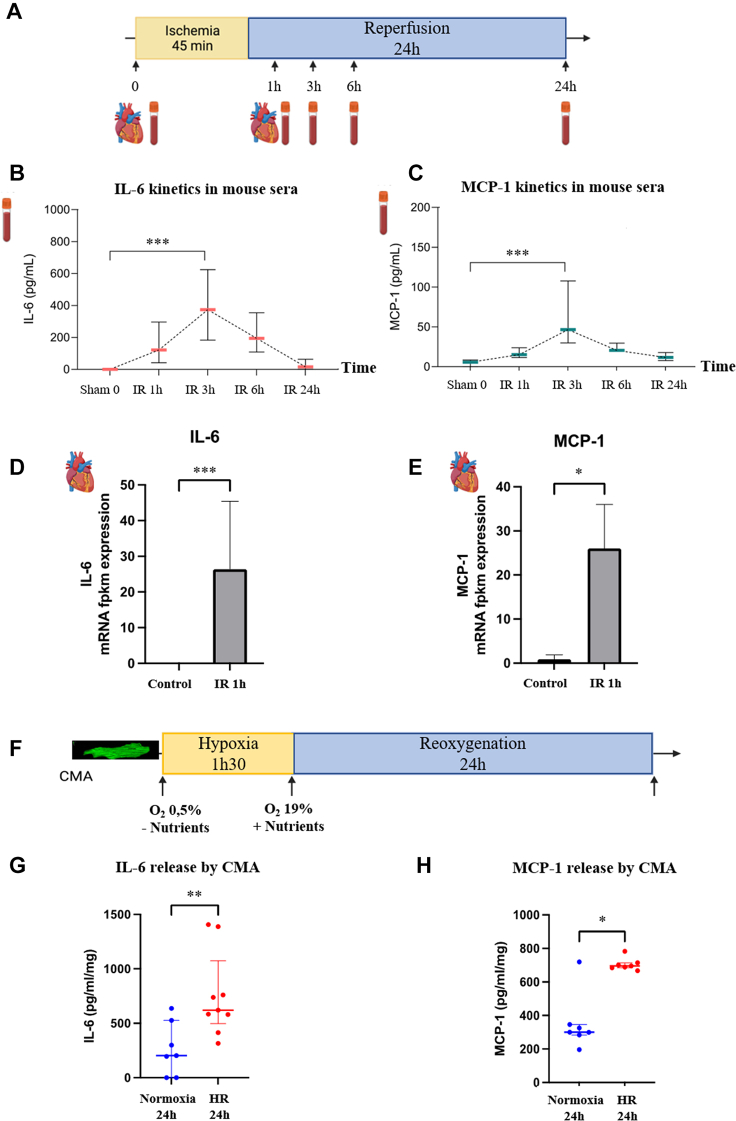
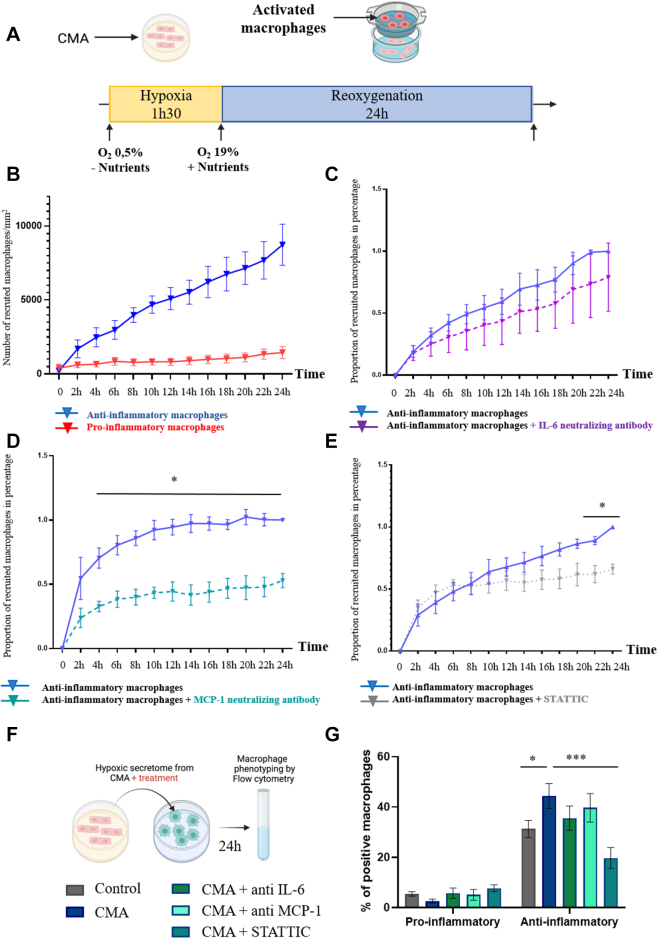
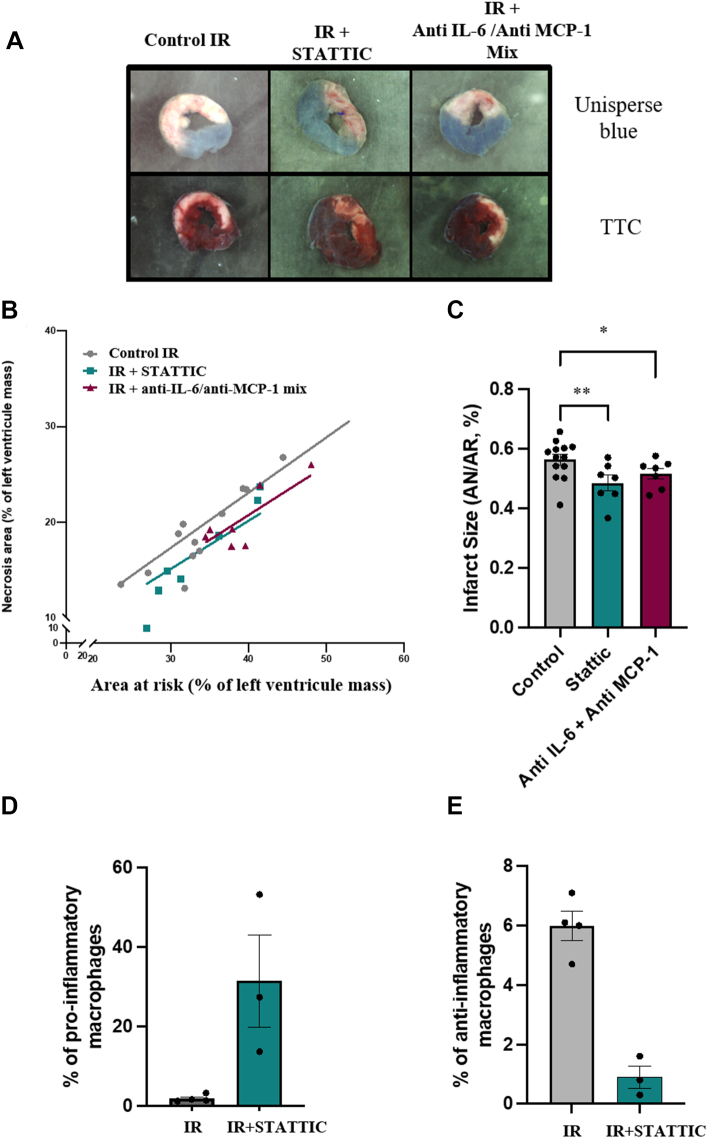
Using a translational approach with an ST-segment myocardial infarction (STEMI) cohort and mouse model of myocardial infarction, we highlighted the role of the secreted IL-6 and MCP-1 cytokines and the STAT3 pathway in heart macrophage recruitment and activation. Cardiac myocytes secrete IL-6 and MCP-1 in response to hypoxic stress, leading to a recruitment and/or polarization of anti-inflammatory macrophages via the STAT3 pathway. In our preclinical model of myocardial infarction, neutralization of IL-6 and MCP-1 or STAT3 pathway reduced infarct size. Together, our data demonstrate that anti-inflammatory macrophages can be deleterious in the acute phase of STEMI.
Keywords: IL-6; MCP-1; STAT3; inflammation; macrophages; myocardial infarction.
© 2024 The Authors.
Conflict of interest statement
This work was supported by “Federation Française de Cardiologie,” and LABEX CORTEX (ANR-11-LABX-0042) and FRM (FD202012010540). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
Cardiac overexpression of monocyte chemoattractant protein-1 in transgenic mice prevents cardiac dysfunction and remodeling after myocardial infarction.Circ Res. 2006 Oct 13;99(8):891-9. doi: 10.1161/01.RES.0000246113.82111.2d. Epub 2006 Sep 21. Circ Res. 2006. PMID: 16990567
-
IL (Interleukin)-10-STAT3-Galectin-3 Axis Is Essential for Osteopontin-Producing Reparative Macrophage Polarization After Myocardial Infarction.Circulation. 2018 Oct 30;138(18):2021-2035. doi: 10.1161/CIRCULATIONAHA.118.035047. Circulation. 2018. PMID: 29967195
-
CCL2/Monocyte Chemoattractant Protein-1 regulates inflammatory responses critical to healing myocardial infarcts.Circ Res. 2005 Apr 29;96(8):881-9. doi: 10.1161/01.RES.0000163017.13772.3a. Epub 2005 Mar 17. Circ Res. 2005. PMID: 15774854
-
Macrophages in myocardial infarction.Am J Physiol Cell Physiol. 2022 Oct 1;323(4):C1304-C1324. doi: 10.1152/ajpcell.00230.2022. Epub 2022 Sep 12. Am J Physiol Cell Physiol. 2022. PMID: 36094436 Free PMC article. Review.
-
The inflammatory response in myocardial infarction.Cardiovasc Res. 2002 Jan;53(1):31-47. doi: 10.1016/s0008-6363(01)00434-5. Cardiovasc Res. 2002. PMID: 11744011 Review.
Cited by
-
Targeting Macrophage Phenotype for Treating Heart Failure: A New Approach.Drug Des Devel Ther. 2024 Nov 5;18:4927-4942. doi: 10.2147/DDDT.S486816. eCollection 2024. Drug Des Devel Ther. 2024. PMID: 39525046 Free PMC article. Review.
References
-
- Mitsis A., Kadoglou N.P.E., Lambadiari V., et al. Prognostic role of inflammatory cytokines and novel adipokines in acute myocardial infarction: an updated and comprehensive review. Cytokine. 2022;153 - PubMed
-
- Bochaton T., Paccalet A., Jeantet P., et al. Heat shock protein 70 as a biomarker of clinical outcomes after STEMI. J Am Coll Cardiol. 2020;75:122–124. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
