

Exercise training improves exercise capacity and quality of life in heart failure with preserved ejection fraction: a systematic review and meta-analysis of randomized controlled trials
- PMID: 38982996
- PMCID: PMC11231943
- DOI: 10.1093/ehjopen/oeae033
Exercise training improves exercise capacity and quality of life in heart failure with preserved ejection fraction: a systematic review and meta-analysis of randomized controlled trials
Abstract
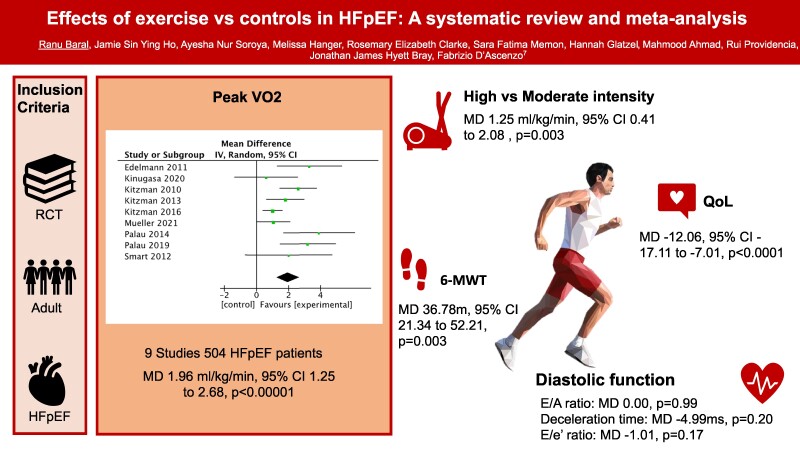
Aims: Heart failure with preserved ejection fraction (HFpEF) is associated with high morbidity and mortality, and there are limited proven therapeutic strategies. Exercise has been shown to be beneficial in several studies. We aimed to evaluate the efficacy of exercise on functional, physiological, and quality-of-life measures.
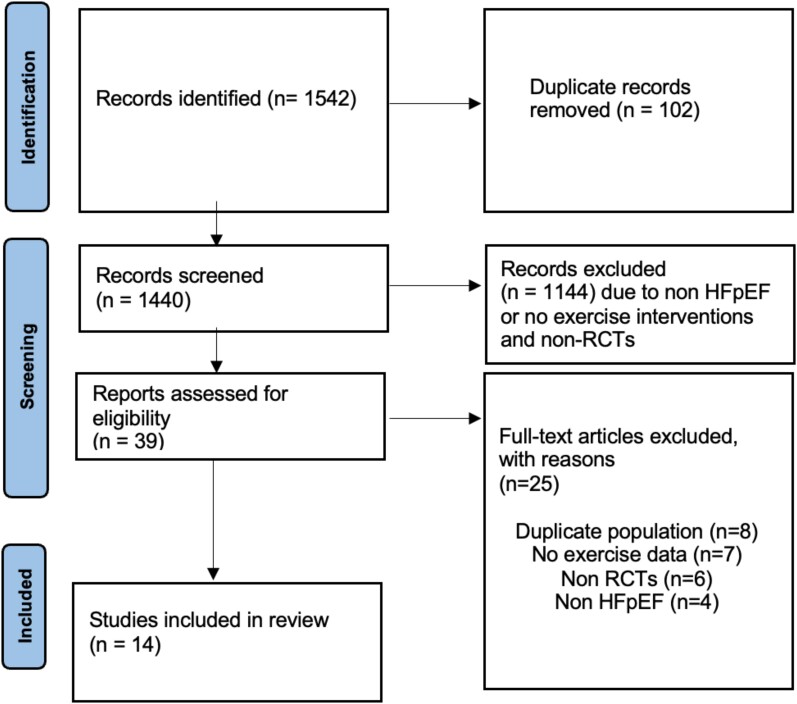
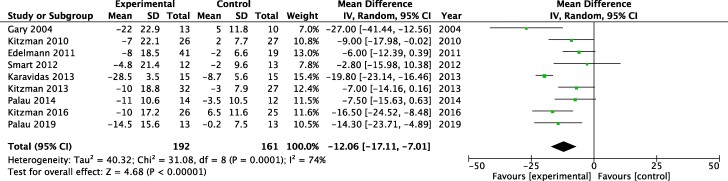
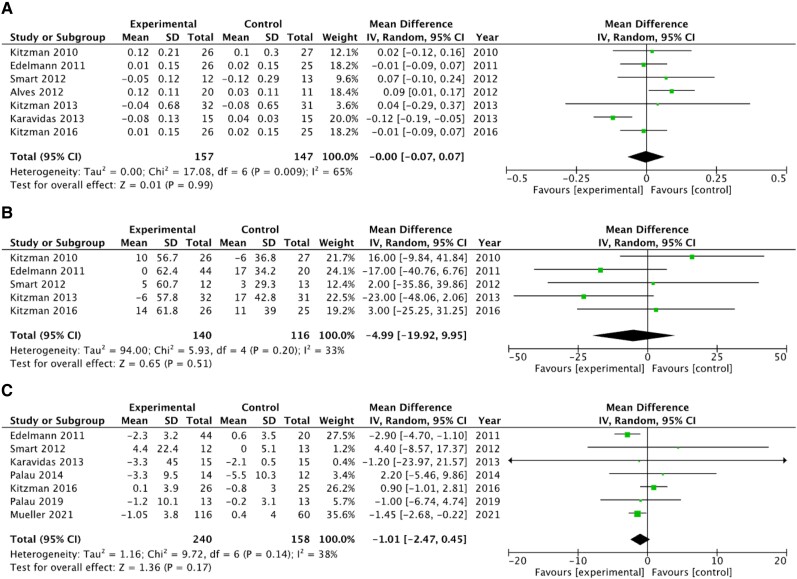
Methods and results: A comprehensive search of Medline and Embase was performed. Randomized controlled trials (RCTs) of adult HFpEF patients with data on exercise intervention were included. Using meta-analysis, we produced pooled mean difference (MD) estimates with 95% confidence intervals (CIs) with Review Manager (RevMan) software for the peak oxygen uptake (VO2), Minnesota living with heart failure (MLWHF) and, other diastolic dysfunction scores. A total of 14 studies on 629 HFpEF patients were included (63.2% female) with a mean age of 68.1 years. Exercise was associated with a significant improvement in the peak VO2 (MD 1.96 mL/kg/min, 95% CI 1.25-2.68; P < 0.00001) and MLWHF score (MD -12.06, 95% CI -17.11 to -7.01; P < 0.00001) in HFpEF. Subgroup analysis showed a small but significant improvement in peak VO2 with high-intensity interval training (HIIT) vs. medium-intensity continuous exercise (MCT; MD 1.25 mL/kg/min, 95% CI 0.41-2.08, P = 0.003).
Conclusion: Exercise increases the exercise capacity and quality of life in HFpEF patients, and high-intensity exercise is associated with a small but statistically significant improvement in exercise capacity than moderate intensity. Further studies with larger participant populations and longer follow-up are needed to confirm these findings and elucidate potential differences between high- and medium-intensity exercise.
Keywords: Exercise training; HFpEF; Heart failure; Heart failure with preserved ejection fraction; Meta-analysis.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: none declared.
Figures


Similar articles
-
High-intensity and moderate-intensity interval training in heart failure with preserved ejection fraction: A meta-analysis of randomized controlled trials.Medicine (Baltimore). 2023 Feb 22;102(8):e33010. doi: 10.1097/MD.0000000000033010. Medicine (Baltimore). 2023. PMID: 36827059 Free PMC article.
-
High-Intensity Interval Training Versus Moderate Continuous Training in Patients With Heart Failure With Preserved Ejection Fraction: A Systematic Review and Meta-analysis.Curr Probl Cardiol. 2023 Aug;48(8):101720. doi: 10.1016/j.cpcardiol.2023.101720. Epub 2023 Mar 24. Curr Probl Cardiol. 2023. PMID: 36967072 Review.
-
Effects of drug and exercise intervention on functional capacity and quality of life in heart failure with preserved ejection fraction: A meta-analysis of randomized controlled trials.Eur J Prev Cardiol. 2016 Jan;23(1):78-85. doi: 10.1177/2047487314564729. Epub 2014 Dec 17. Eur J Prev Cardiol. 2016. PMID: 25520380
-
Supervised exercise training in heart failure with preserved ejection fraction: A systematic review and meta-analysis of randomized controlled trials.Curr Probl Cardiol. 2024 Apr;49(4):102426. doi: 10.1016/j.cpcardiol.2024.102426. Epub 2024 Feb 3. Curr Probl Cardiol. 2024. PMID: 38311273 Review.
-
Effects of exercise training on cardiac function, exercise capacity, and quality of life in heart failure with preserved ejection fraction: a meta-analysis of randomized controlled trials.Heart Fail Rev. 2019 Jul;24(4):535-547. doi: 10.1007/s10741-019-09774-5. Heart Fail Rev. 2019. PMID: 31032533
Cited by
-
Importance of health-related quality of gain with exercise training in preserved ejection fraction heart failure.Eur Heart J Open. 2024 Oct 17;4(6):oeae091. doi: 10.1093/ehjopen/oeae091. eCollection 2024 Nov. Eur Heart J Open. 2024. PMID: 39493572 Free PMC article. No abstract available.
References
-
- Cook C, Cole G, Asaria P, Jabbour R, Francis DP. The annual global economic burden of heart failure. Int J Cardiol 2014;171:368–376. - PubMed
-
- Golla MSG, Hajouli S, Ludhwani D. Heart failure and ejection fraction. StatPearls. 2024. https://www.ncbi.nlm.nih.gov/books/NBK553115/ (10 June 2024).
-
- Cheng RK, Cox M, Neely ML, Heidenreich PA, Bhatt DL, Eapen ZJ, Hernandez AF, Butler J, Yancy CW, Fonarow GC. Outcomes in patients with heart failure with preserved, borderline, and reduced ejection fraction in the Medicare population. Am Heart J 2014;168:721–730.e3. - PubMed
-
- Lewis EF, Lamas GA, O’Meara E, Granger CB, Dunlap ME, McKelvie RS, Probstfield JL, Young JB, Michelson EL, Halling K, Carlsson J, Olofsson B, McMurray JJV, Yusuf S, Swedberg K, Pfeffer MA. Characterization of health-related quality of life in heart failure patients with preserved versus low ejection fraction in CHARM. Eur J Heart Fail 2007;9:83–91. - PubMed
LinkOut - more resources
Full Text Sources
