

The potential role of serum amyloid A as biomarker of rheumatic diseases: a systematic review and meta-analysis
- PMID: 38951267
- PMCID: PMC11217051
- DOI: 10.1007/s10238-024-01413-0
The potential role of serum amyloid A as biomarker of rheumatic diseases: a systematic review and meta-analysis
Abstract
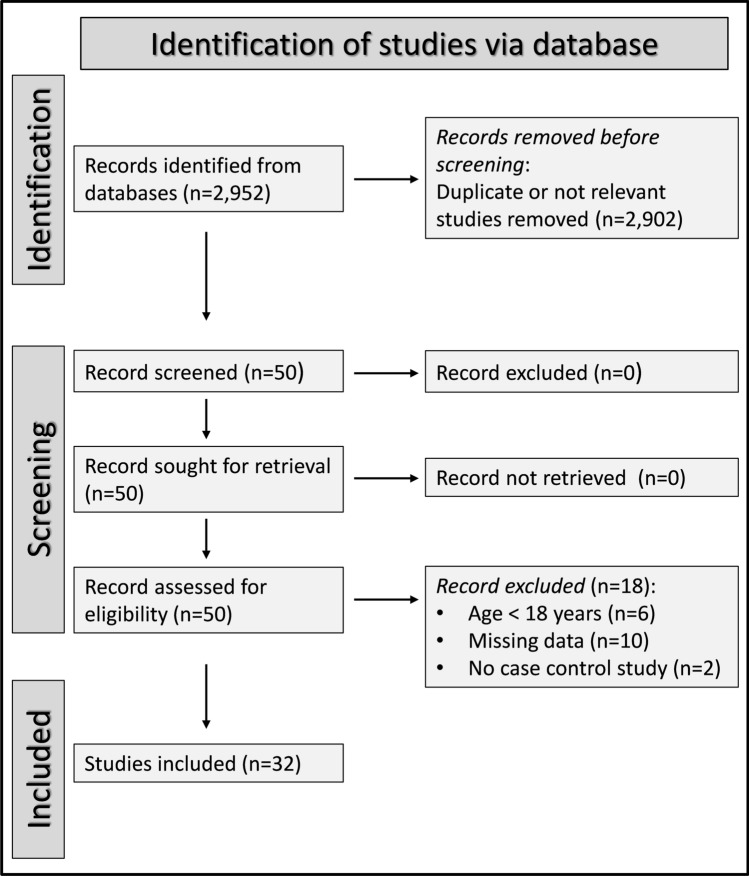
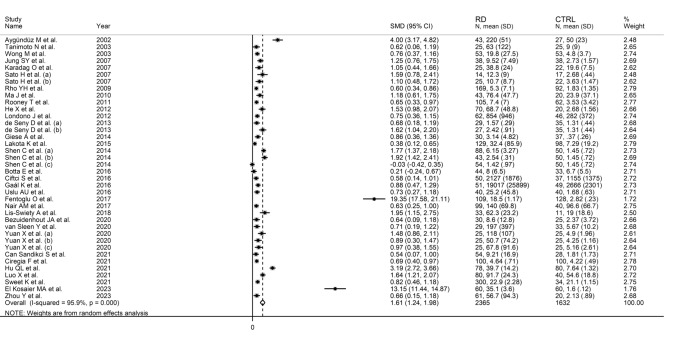
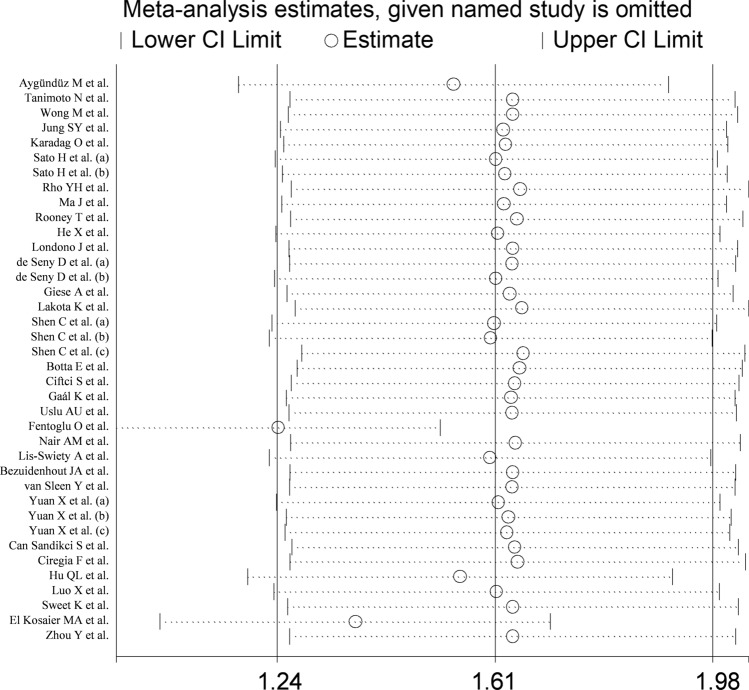
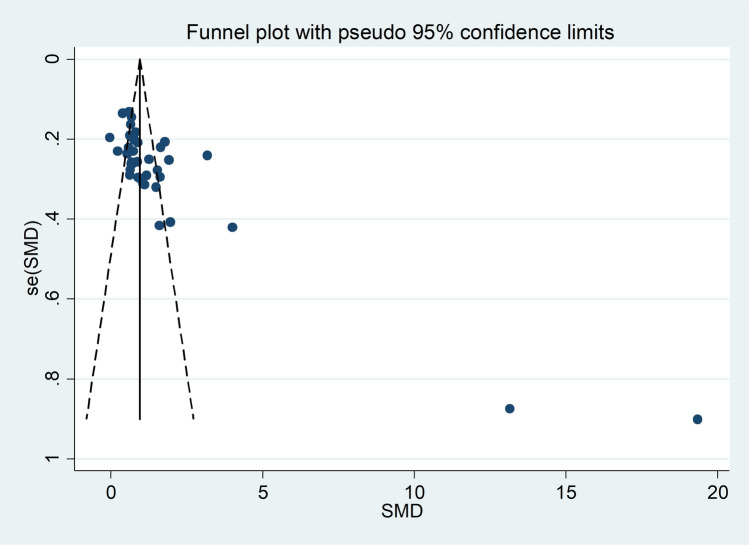
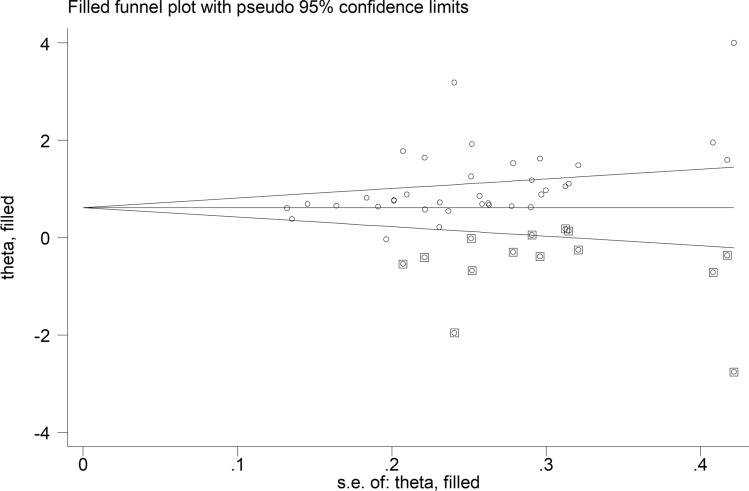
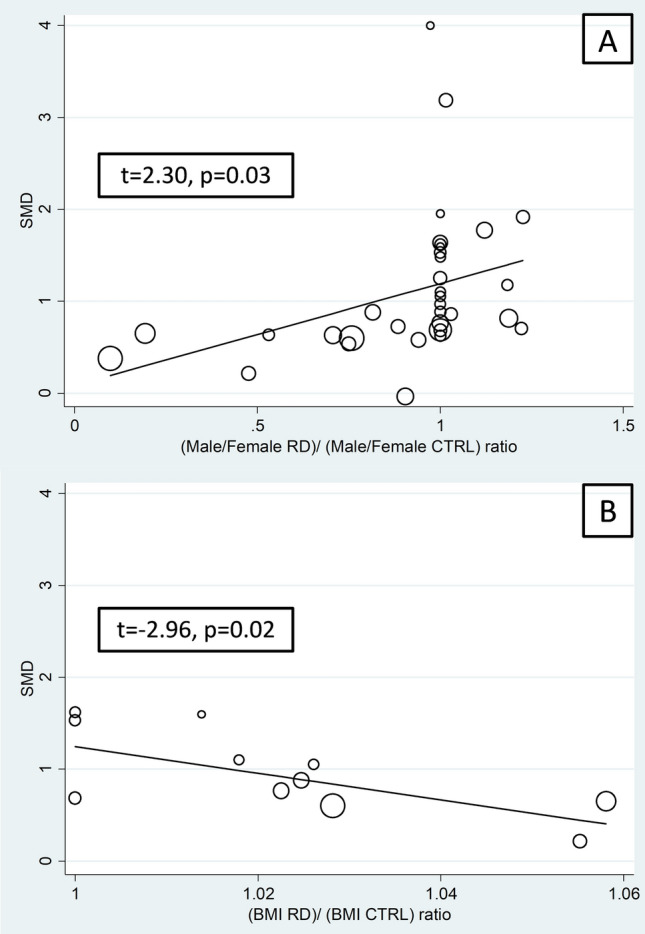
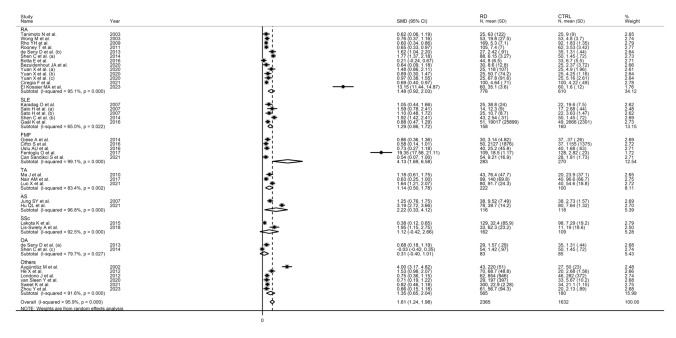
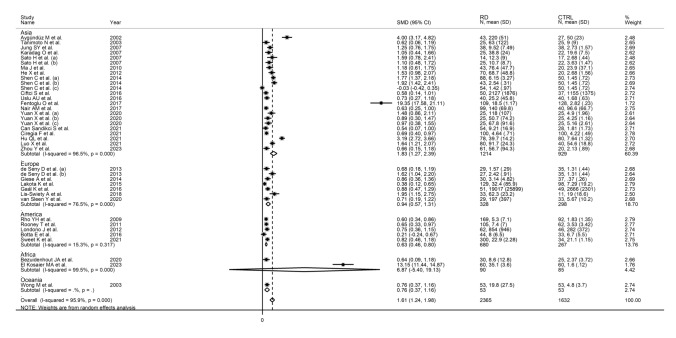
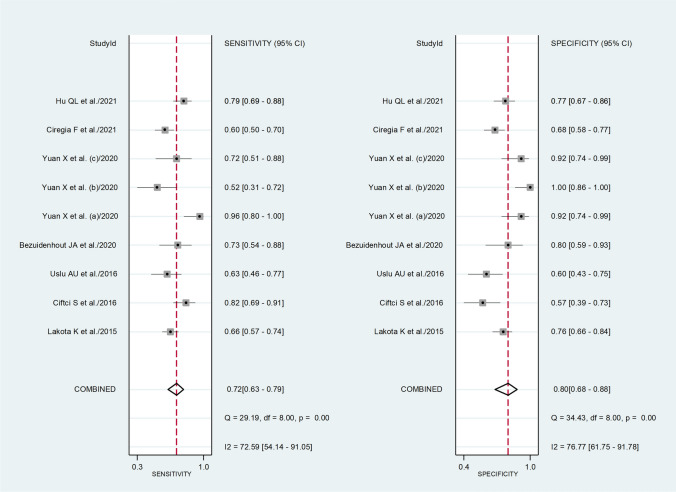
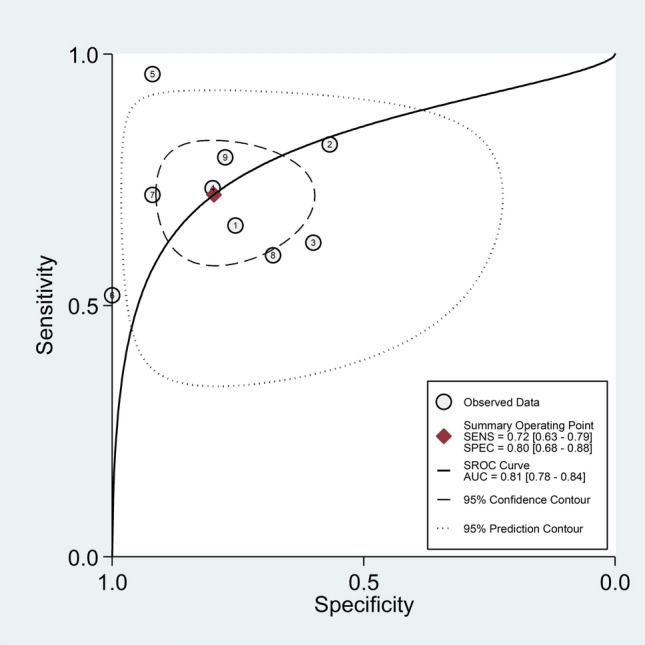
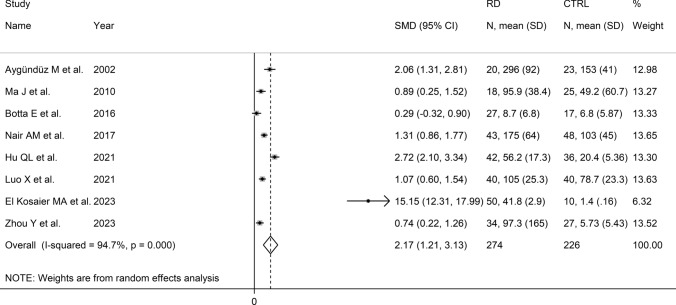
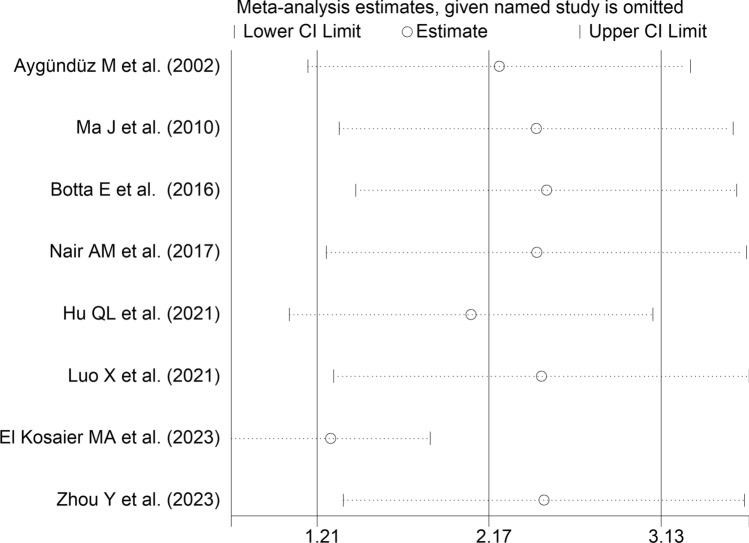
The identification of novel, robust biomarkers for the diagnosis of rheumatic diseases (RDs) and the presence of active disease might facilitate early treatment and the achievement of favourable long-term outcomes. We conducted a systematic review and meta-analysis of studies investigating the acute phase reactant, serum amyloid A (SAA), in RD patients and healthy controls to appraise its potential as diagnostic biomarker. We searched PubMed, Scopus, and Web of Science from inception to 10 April 2024 for relevant studies. We evaluated the risk of bias and the certainty of evidence using the JBI Critical Appraisal Checklist and GRADE, respectively (PROSPERO registration number: CRD42024537418). In 32 studies selected for analysis, SAA concentrations were significantly higher in RD patients compared to controls (SMD = 1.61, 95% CI 1.24-1.98, p < 0.001) and in RD patients with active disease compared to those in remission (SMD = 2.17, 95% CI 1.21-3.13, p < 0.001). Summary receiving characteristics curve analysis showed a good diagnostic accuracy of SAA for the presence of RDs (area under the curve = 0.81, 95% CI 0.78-0.84). The effect size of the differences in SAA concentrations between RD patients and controls was significantly associated with sex, body mass index, type of RD, and study country. Pending the conduct of prospective studies in different types of RDs, the results of this systematic review and meta-analysis suggest that SAA is a promising biomarker for the diagnosis of RDs and active disease.
Keywords: Active disease; Autoimmunity; Biomarkers; Diagnostic accuracy; Inflammation; Rheumatic diseases; Serum amyloid A.
© 2024. The Author(s).
Conflict of interest statement
The authors have no relevant financial or non-financial interests to disclose.
Figures
Similar articles
-
Falls prevention interventions for community-dwelling older adults: systematic review and meta-analysis of benefits, harms, and patient values and preferences.Syst Rev. 2024 Nov 26;13(1):289. doi: 10.1186/s13643-024-02681-3. Syst Rev. 2024. PMID: 39593159 Free PMC article.
-
A systematic review and meta-analysis of the endothelial-immune candidate biomarker endoglin in rheumatic diseases.Clin Exp Med. 2024 Nov 13;25(1):4. doi: 10.1007/s10238-024-01519-5. Clin Exp Med. 2024. PMID: 39535678 Free PMC article. Review.
-
Undernutrition as a risk factor for tuberculosis disease.Cochrane Database Syst Rev. 2024 Jun 11;6(6):CD015890. doi: 10.1002/14651858.CD015890.pub2. Cochrane Database Syst Rev. 2024. PMID: 38860538 Free PMC article. Review.
-
Plasmapheresis to remove amyloid fibrin(ogen) particles for treating the post-COVID-19 condition.Cochrane Database Syst Rev. 2023 Jul 26;7(7):CD015775. doi: 10.1002/14651858.CD015775. Cochrane Database Syst Rev. 2023. PMID: 37491597 Free PMC article. Review.
-
Genedrive kit for detecting single nucleotide polymorphism m.1555A>G in neonates and their mothers: a systematic review and cost-effectiveness analysis.Health Technol Assess. 2024 Oct;28(75):1-75. doi: 10.3310/TGAC4201. Health Technol Assess. 2024. PMID: 39487741 Free PMC article.
References
-
- Chauhan R, Raina V, Nandi SP. Prevalence of autoimmune diseases and its challenges in diagnosis. Crit Rev Immunol. 2019;39(3):189–201. 10.1615/CritRevImmunol.2019031798. - PubMed
-
- Lenti MV, Rossi CM, Melazzini F, et al. Seronegative autoimmune diseases: a challenging diagnosis. Autoimmun Rev. 2022;21(9): 103143. 10.1016/j.autrev.2022.103143. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
