

Does clinical T1N0 GGN really require checking for distant metastasis during initial staging for lung cancer?
- PMID: 38831467
- PMCID: PMC11149246
- DOI: 10.1186/s40644-024-00714-7
Does clinical T1N0 GGN really require checking for distant metastasis during initial staging for lung cancer?
Abstract
Background: Accurate clinical staging is crucial for selection of optimal oncological treatment strategies in non-small cell lung cancer (NSCLC). Although brain MRI, bone scintigraphy and whole-body PET/CT play important roles in detecting distant metastases, there is a lack of evidence regarding the indication for metastatic staging in early NSCLCs, especially ground-grass nodules (GGNs). Our aim was to determine whether checking for distant metastasis is required in cases of clinical T1N0 GGN.
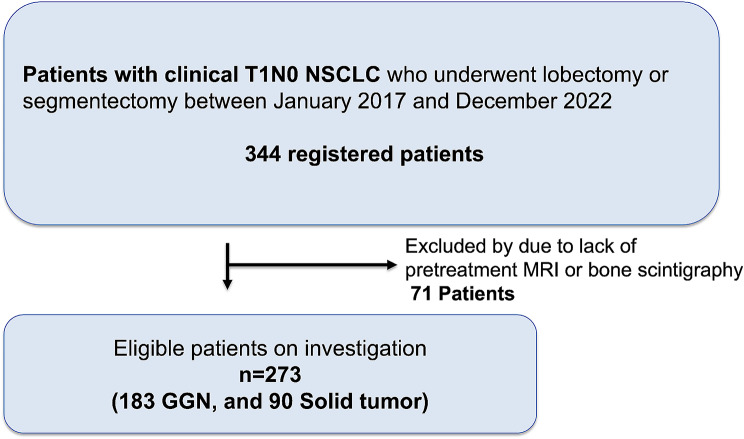
Methods: This was a retrospective study of initial staging using imaging tests in patients who had undergone complete surgical R0 resection for clinical T1N0 Stage IA NSCLC.
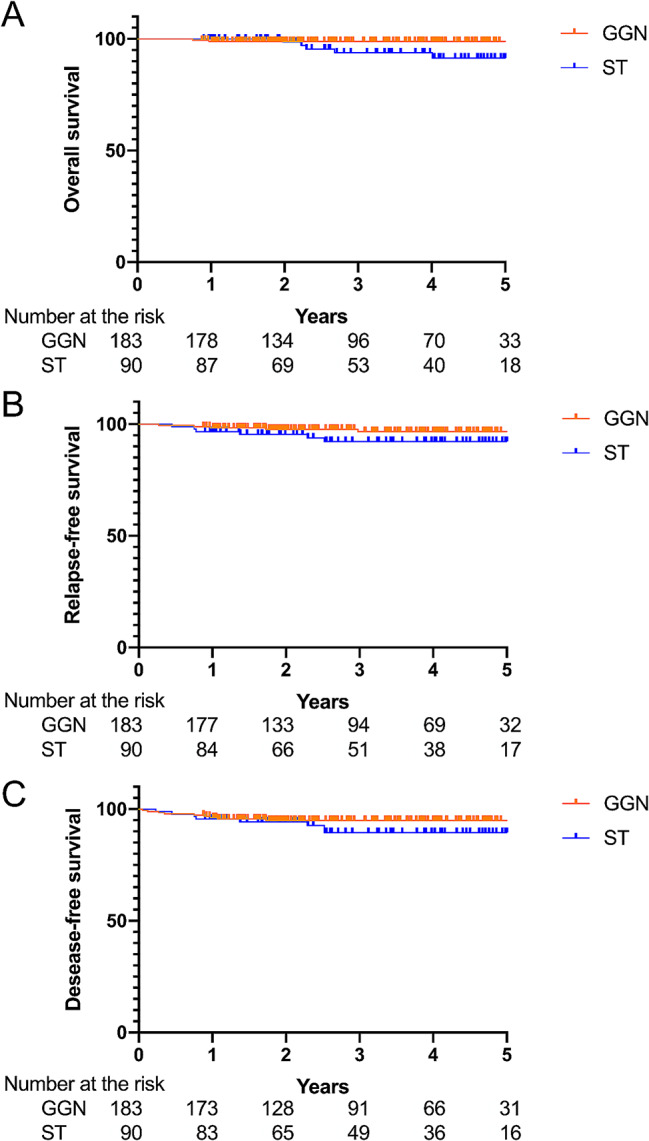
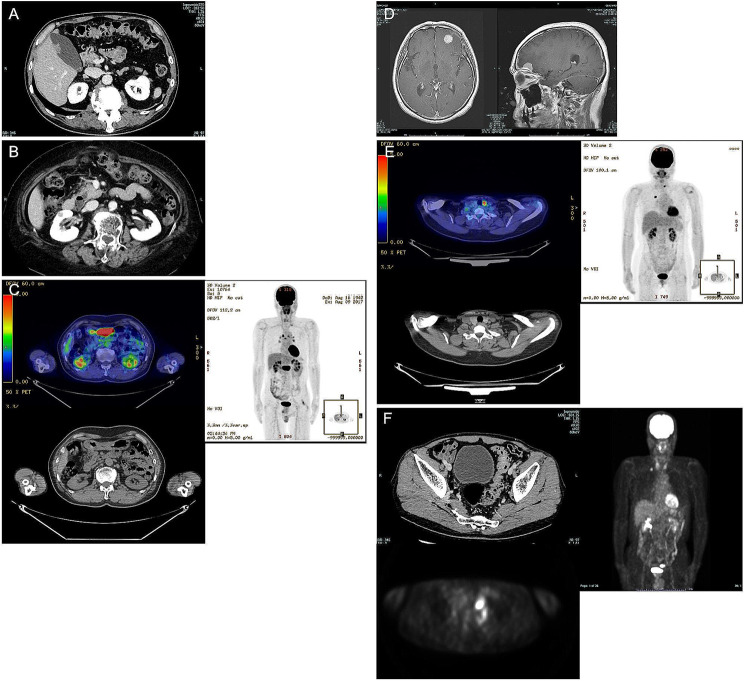
Results: A total of 273 patients with cT1N0 GGNs (n = 183) or cT1N0 solid tumors (STs, n = 90) were deemed eligible. No cases of distant metastasis were detected on initial routine imaging evaluations. Among all cT1N0M0 cases, there were 191 incidental findings on various modalities (128 in the GGN). Most frequently detected on brain MRI was cerebral leukoaraiosis, which was found in 98/273 (35.9%) patients, while cerebral infarction was detected in 12/273 (4.4%) patients. Treatable neoplasms, including brain meningioma and thyroid, gastric, renal and colon cancers were also detected on PET/CT (and/or MRI). Among those, 19 patients were diagnosed with a treatable disease, including other-site cancers curable with surgery.
Conclusions: Extensive staging (MRI, scintigraphy, PET/CT etc.) for distant metastasis is not required for patients diagnosed with clinical T1N0 GGNs, though various imaging modalities revealed the presence of adventitious diseases with the potential to increase surgical risks, lead to separate management, and worsen patient outcomes, especially in elderly patients. If clinically feasible, it could be considered to complement staging with whole-body procedures including PET/CT.
Keywords: Diagnostic screening programs; Incidental findings; Lung neoplasms; Neoplasm staging.
© 2024. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
Similar articles
-
Significance of Brain Imaging for Staging in Patients With Clinical Stage T1-2 N0 Non-Small-Cell Lung Cancer on Positron Emission Tomography/Computed Tomography.Clin Lung Cancer. 2021 Nov;22(6):562-569. doi: 10.1016/j.cllc.2021.06.004. Epub 2021 Jun 13. Clin Lung Cancer. 2021. PMID: 34253472
-
Utility of FDG PET/CT for Preoperative Staging of Non-Small Cell Lung Cancers Manifesting as Subsolid Nodules With a Solid Portion of 3 cm or Smaller.AJR Am J Roentgenol. 2020 Mar;214(3):514-523. doi: 10.2214/AJR.19.21811. Epub 2019 Dec 17. AJR Am J Roentgenol. 2020. PMID: 31846374
-
Preoperative staging of non-small-cell lung cancer: comparison of whole-body diffusion-weighted magnetic resonance imaging and 18F-fluorodeoxyglucose-positron emission tomography/computed tomography.Eur Radiol. 2012 Dec;22(12):2859-67. doi: 10.1007/s00330-012-2542-y. Epub 2012 Jul 9. Eur Radiol. 2012. PMID: 22772365
-
A two-way comparison of whole-body 18FDG PET-CT and whole-body contrast-enhanced MRI for distant metastasis staging in patients with malignant tumors: a meta-analysis of 13 prospective studies.Ann Palliat Med. 2020 Mar;9(2):247-255. doi: 10.21037/apm.2020.02.30. Epub 2020 Mar 18. Ann Palliat Med. 2020. PMID: 32233618 Review.
-
Hybrid PET/MRI in non-small cell lung cancer (NSCLC) and lung nodules-a literature review.Eur J Nucl Med Mol Imaging. 2021 Feb;48(2):584-591. doi: 10.1007/s00259-020-04955-z. Epub 2020 Jul 27. Eur J Nucl Med Mol Imaging. 2021. PMID: 32719914 Review.
References
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: non-small cell lung cancer [Internet]. Fort Washington: National Comprehensive Cancer Network. 2023. https://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed March 10, 2023.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
