

Chronic Obstructive Pulmonary Disease Exacerbations Increase the Risk of Subsequent Cardiovascular Events: A Longitudinal Analysis of the COPDGene Study
- PMID: 38818936
- PMCID: PMC11255614
- DOI: 10.1161/JAHA.123.033882
Chronic Obstructive Pulmonary Disease Exacerbations Increase the Risk of Subsequent Cardiovascular Events: A Longitudinal Analysis of the COPDGene Study
Abstract
Background: Cardiovascular disease (CVD) is the most important comorbidity in patients with chronic obstructive pulmonary disease (COPD). COPD exacerbations not only contribute to COPD progression but may also elevate the risk of CVD. This study aimed to determine whether COPD exacerbations increase the risk of subsequent CVD events using up to 15 years of prospective longitudinal follow-up data from the COPDGene (Genetic Epidemiology of Chronic Obstructive Pulmonary Disease) study.
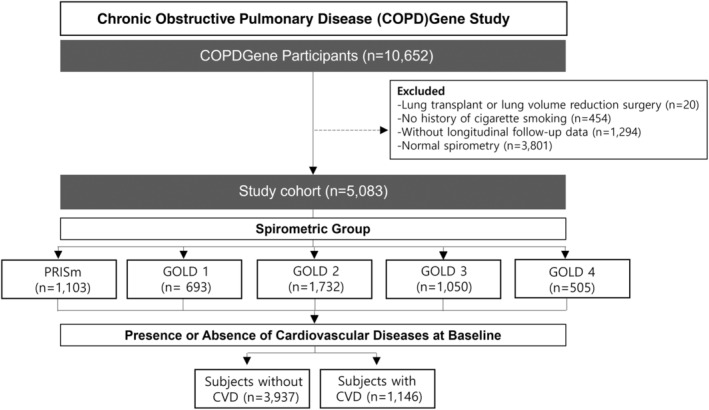
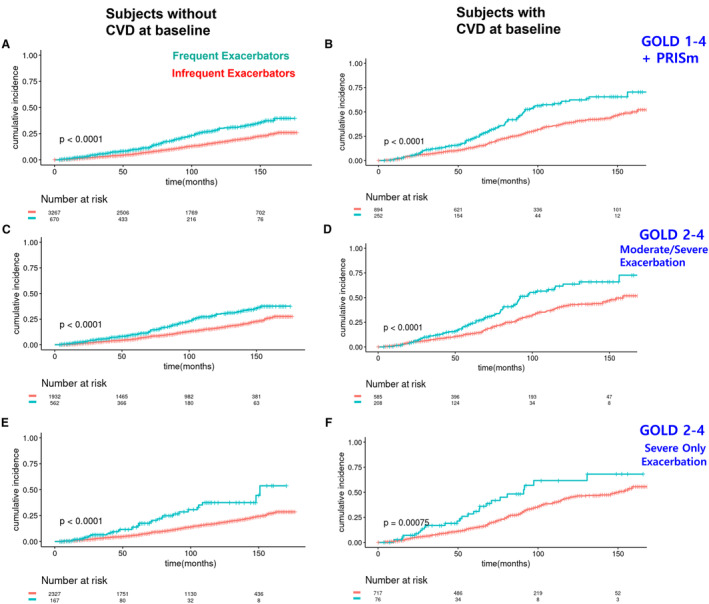
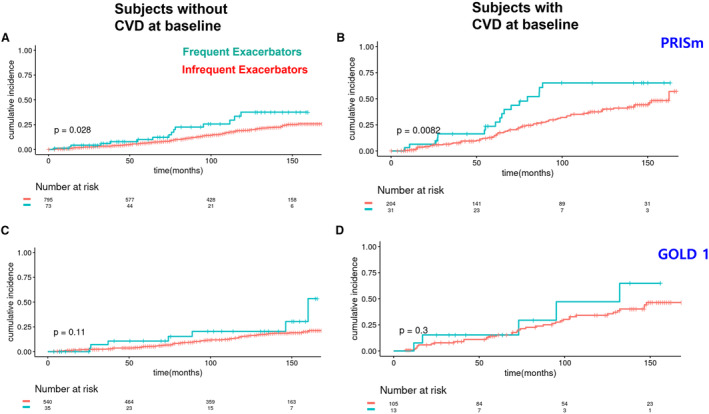
Methods and results: The COPDGene study is a large, multicenter, longitudinal investigation of COPD, including subjects at enrollment aged 45 to 80 years with a minimum of 10 pack-years of smoking history. Cox proportional hazards models and Kaplan-Meier survival curves were used to assess the risk of a composite end point of CVD based on the COPD exacerbation rate. Frequent exacerbators exhibited a higher cumulative incidence of composite CVD end points than infrequent exacerbators, irrespective of the presence of CVD at baseline. After adjusting for covariates, frequent exacerbators still maintained higher hazard ratios (HRs) than the infrequent exacerbator group (without CVD: HR, 1.81 [95% CI, 1.47-2.22]; with CVD: HR, 1.92 [95% CI, 1.51-2.44]). This observation remained consistently significant in moderate to severe COPD subjects and the preserved ratio impaired spirometry population. In the mild COPD population, frequent exacerbators showed a trend toward more CVD events.
Conclusions: COPD exacerbations are associated with an increased risk of subsequent cardiovascular events in subjects with and without preexisting CVD. Patients with COPD experiencing frequent exacerbations may necessitate careful monitoring and additional management for subsequent potential CVD.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT00608764.
Keywords: COPD exacerbation; cardiovascular events; chronic obstructive pulmonary disease; clinical epidemiology; preserved ratio impaired spirometry.
Figures
Similar articles
-
Stability of the frequent COPD exacerbator in the general population: A Danish nationwide register-based study.NPJ Prim Care Respir Med. 2017 Apr 17;27(1):25. doi: 10.1038/s41533-017-0029-7. NPJ Prim Care Respir Med. 2017. PMID: 28416794 Free PMC article.
-
Cardiovascular events after exacerbations of chronic obstructive pulmonary disease: Results from the EXAcerbations of COPD and their OutcomeS in CardioVascular diseases study in Italy.Eur J Intern Med. 2024 Sep;127:97-104. doi: 10.1016/j.ejim.2024.04.021. Epub 2024 May 9. Eur J Intern Med. 2024. PMID: 38729787
-
Statin Use and the Risk of Subsequent Hospitalized Exacerbations in COPD Patients with Frequent Exacerbations.Int J Chron Obstruct Pulmon Dis. 2020 Feb 10;15:289-299. doi: 10.2147/COPD.S229047. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32103928 Free PMC article.
-
Clinical Epidemiology of COPD: Insights From 10 Years of the COPDGene Study.Chest. 2019 Aug;156(2):228-238. doi: 10.1016/j.chest.2019.04.135. Epub 2019 May 30. Chest. 2019. PMID: 31154041 Free PMC article. Review.
-
Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD).Cochrane Database Syst Rev. 2013 Nov 28;(11):CD009764. doi: 10.1002/14651858.CD009764.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2018 Oct 30;10:CD009764. doi: 10.1002/14651858.CD009764.pub3. PMID: 24288145 Updated. Review.
Cited by
-
Aspirin reduces the mortality risk of patients with community-acquired pneumonia: a retrospective propensity-matched analysis of the MIMIC-IV database.Front Pharmacol. 2024 Sep 13;15:1402386. doi: 10.3389/fphar.2024.1402386. eCollection 2024. Front Pharmacol. 2024. PMID: 39346559 Free PMC article.
-
Exploring the Impact of Inhaled Corticosteroids on Endothelial Function in Chronic Obstructive Pulmonary Disease Patients Undergoing Pulmonary Rehabilitation.J Clin Med. 2024 Sep 27;13(19):5749. doi: 10.3390/jcm13195749. J Clin Med. 2024. PMID: 39407809 Free PMC article.
References
-
- Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ, Benziger CP, et al. Global burden of cardiovascular diseases and risk factors, 1990‐2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010 - DOI - PMC - PubMed
-
- Divo M, Cote C, de Torres JP, Casanova C, Marin JM, Pinto‐Plata V, Zulueta J, Cabrera C, Zagaceta J, Hunninghake G, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186:155–161. doi: 10.1164/rccm.201201-0034OC - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
