

Multilevel Analysis of the Neovascularization and Integration Process of a Nonvascularized Rectus Fascia Transplantation
- PMID: 38757048
- PMCID: PMC11098214
- DOI: 10.1097/TXD.0000000000001624
Multilevel Analysis of the Neovascularization and Integration Process of a Nonvascularized Rectus Fascia Transplantation
Abstract
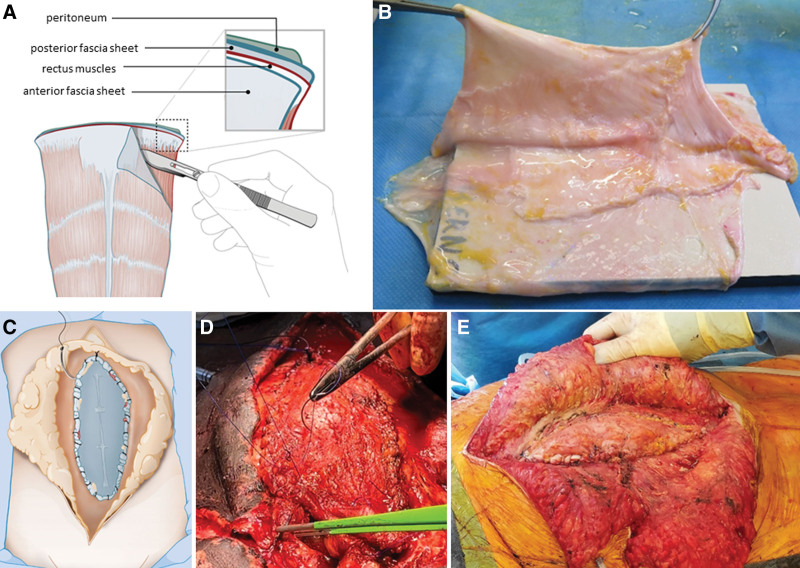
Background: Failure to close the abdominal wall after intestinal transplantation (ITx) or multivisceral Tx remains a surgical challenge. An attractive method is the use of nonvascularized rectus fascia (NVRF) in which both layers of the donor abdominal rectus fascia are used as an inlay patch without vascular anastomosis. How this graft integrates over time remains unknown. The study aims to provide a multilevel analysis of the neovascularization and integration process of the NVRF.
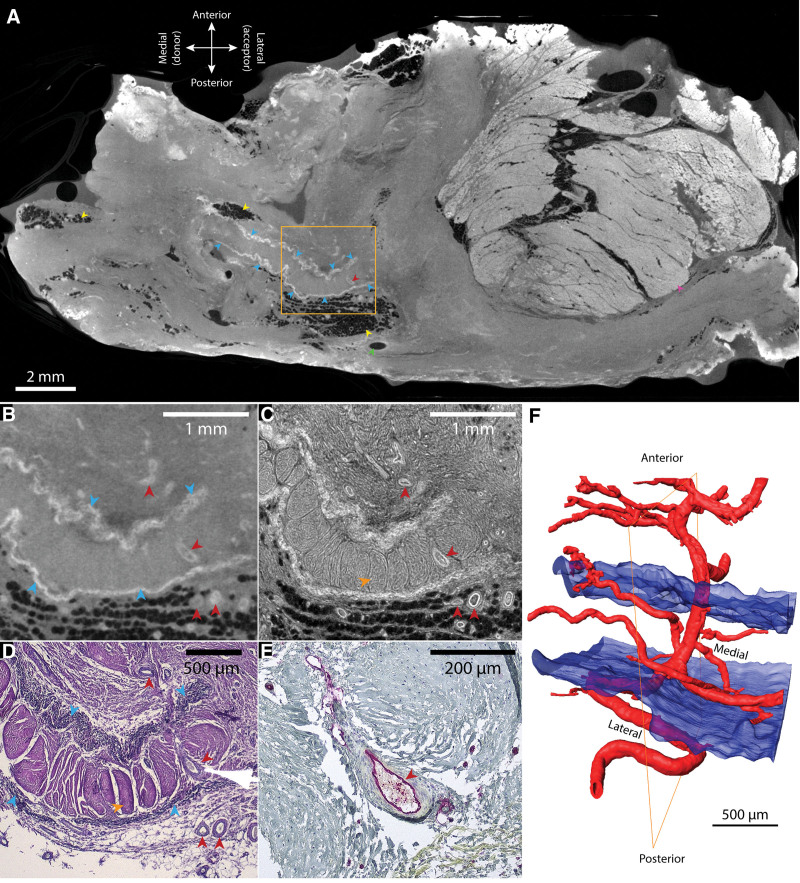
Methods: Three NVRF-Tx were performed after ITx. Clinical, radiological, histological, and immunological data were analyzed to get insights into the neovascularization and integration process of the NVRF. Moreover, cryogenic contrast-enhanced microfocus computed tomography (microCT) analysis was used for detailed reconstruction of the vasculature in and around the NVRF (3-dimensional histology).
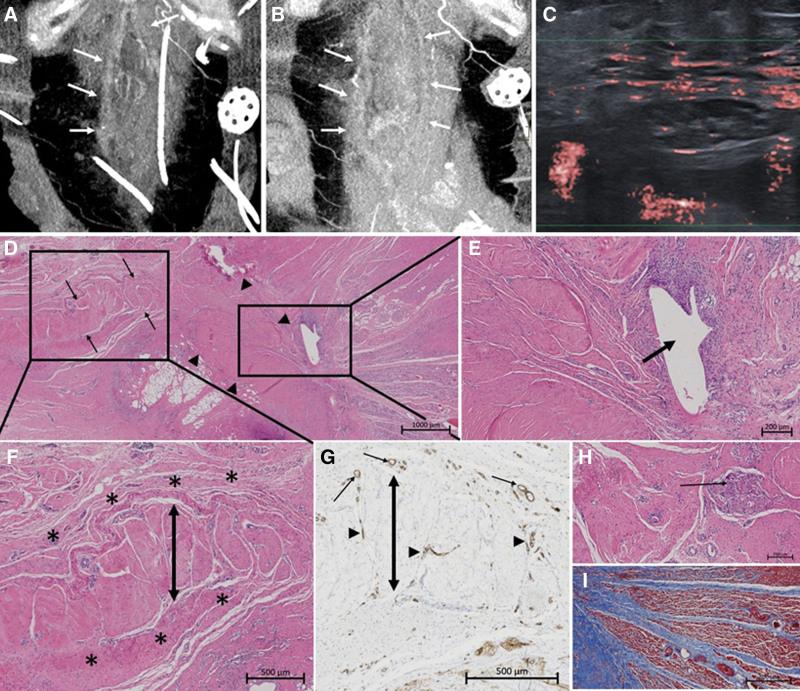
Results: Two men (31- and 51-y-old) and 1 woman (49-y-old) underwent 2 multivisceral Tx and 1 combined liver-ITx, respectively. A CT scan showed contrast enhancement around the fascia graft at 5 days post-Tx. At 6 weeks, newly formed blood vessels were visualized around the graft with Doppler ultrasound. Biopsies at 2 weeks post-Tx revealed inflammation around the NVRF and early fibrosis. At 6 months, classical 2-dimensional histological analysis of a biopsy confirmed integration of the fascia graft with strong fibrotic reaction without signs of rejection. A cryogenic contrast-enhanced microCT scan of the same biopsy revealed the presence of microvasculature, enveloping and penetrating the donor fascia.
Conclusions: We showed clinical, histological, and microCT evidence of the neovascularization and integration process of the NVRF after Tx.
Copyright © 2024 The Author(s). Transplantation Direct. Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Abdominal Wall Closure in Intestinal and Multivisceral Transplantation: A State-Of-The-Art Review of Vascularized Abdominal Wall and Nonvascularized Rectus Fascia Transplantation.Gastroenterol Clin North Am. 2024 Jun;53(2):265-279. doi: 10.1016/j.gtc.2023.12.001. Epub 2024 Jan 25. Gastroenterol Clin North Am. 2024. PMID: 38719377 Review.
-
Long-Term Outcomes of Intestinal and Multivisceral Transplantation at a Single Center in Argentina.Transplant Proc. 2016 Mar;48(2):457-62. doi: 10.1016/j.transproceed.2015.12.066. Transplant Proc. 2016. PMID: 27109978
-
Use of the abdominal rectus fascia as a nonvascularized allograft for abdominal wall closure after liver, intestinal, and multivisceral transplantation.Transplantation. 2009 Jun 27;87(12):1884-8. doi: 10.1097/TP.0b013e3181a7697a. Transplantation. 2009. PMID: 19543069
-
Allotransplantation of donor rectus fascia for abdominal wall closure in transplant patients: A systematic review.Transplant Rev (Orlando). 2021 Dec;35(4):100634. doi: 10.1016/j.trre.2021.100634. Epub 2021 Jun 4. Transplant Rev (Orlando). 2021. PMID: 34147948 Review.
-
Use of Nonvascularized Fascia in Liver Transplantation.Transplant Proc. 2020 Jun;52(5):1468-1471. doi: 10.1016/j.transproceed.2020.01.081. Epub 2020 Mar 21. Transplant Proc. 2020. PMID: 32204902
Cited by
-
Critical Considerations for Expanding Indications for Nonvascularized Rectus Fascia Transplantation: Clarifying Definitions, Techniques, and Immunogenicity.Transplant Direct. 2024 Nov 15;10(12):e1739. doi: 10.1097/TXD.0000000000001739. eCollection 2024 Dec. Transplant Direct. 2024. PMID: 39563726 Free PMC article. No abstract available.
References
-
- Cloonan MR, Fortina CA, Mercer DF, et al. . Failure of abdominal wall closure after intestinal transplantation: identifying high-risk recipients. Clin Transplant. 2019;33:e13713. - PubMed
-
- Janssen Y, Van De Winkel N, Pirenne J, et al. . Allotransplantation of donor rectus fascia for abdominal wall closure in transplant patients: a systematic review. Transplant Rev (Orlando). 2021;35:100634. - PubMed
-
- Ceulemans LJ, Deferm NP, Miserez M, et al. . The role of osmotic self-inflatable tissue expanders in intestinal transplant candidates. Transplant Rev (Orlando). 2016;30:212–217. - PubMed
-
- Farinelli PA, Rubio JS, Padín JM, et al. . Use of nonvascularized abdominal rectus fascia after liver, small bowel, and multiorgan transplantation: long-term follow-up of a single-center series. Transplant Proc. 2017;49:1810–1814. - PubMed
-
- Gerlach UA, Pascher A. Technical advances for abdominal wall closure after intestinal and multivisceral transplantation. Curr Opin Organ Transplant. 2012;17:258–267. - PubMed
LinkOut - more resources
Full Text Sources
