

Tibial Cortex Transverse Transport Facilitates Severe Diabetic Foot Wound Healing via HIF-1α-Induced Angiogenesis
- PMID: 38707956
- PMCID: PMC11070162
- DOI: 10.2147/JIR.S456590
Tibial Cortex Transverse Transport Facilitates Severe Diabetic Foot Wound Healing via HIF-1α-Induced Angiogenesis
Abstract
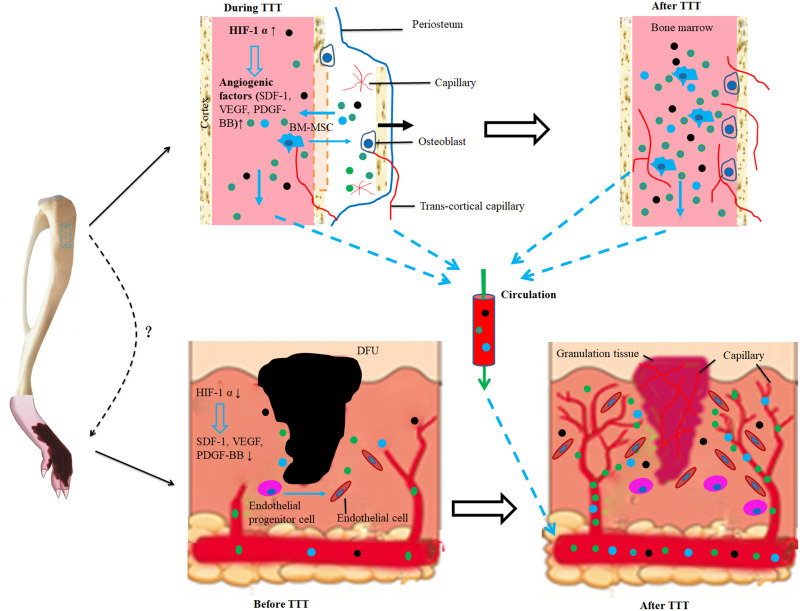
Purpose: Management of severe diabetic foot ulcers (DFUs) remains challenging. Tibial cortex transverse transport (TTT) facilitates healing and limb salvage in patients with recalcitrant DFUs. However, the underlying mechanism is largely unknown, necessitating the establishment of an animal model and mechanism exploration.
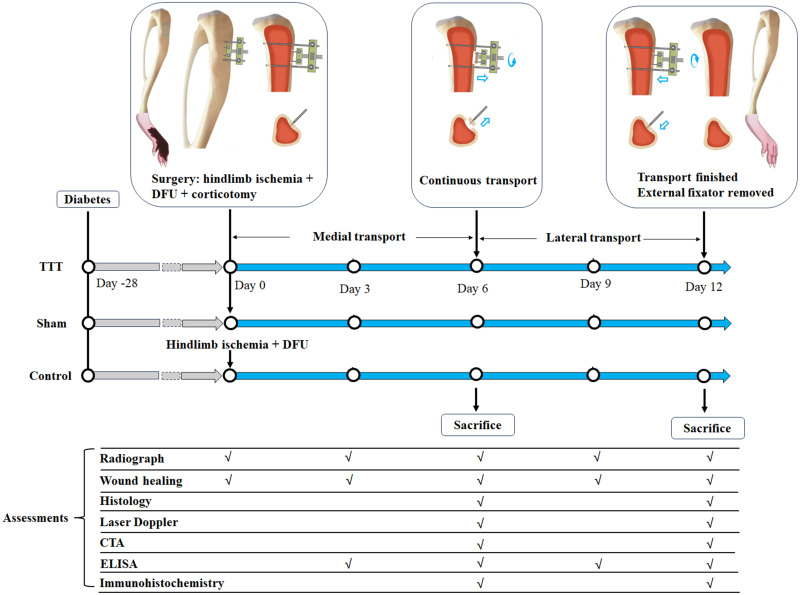
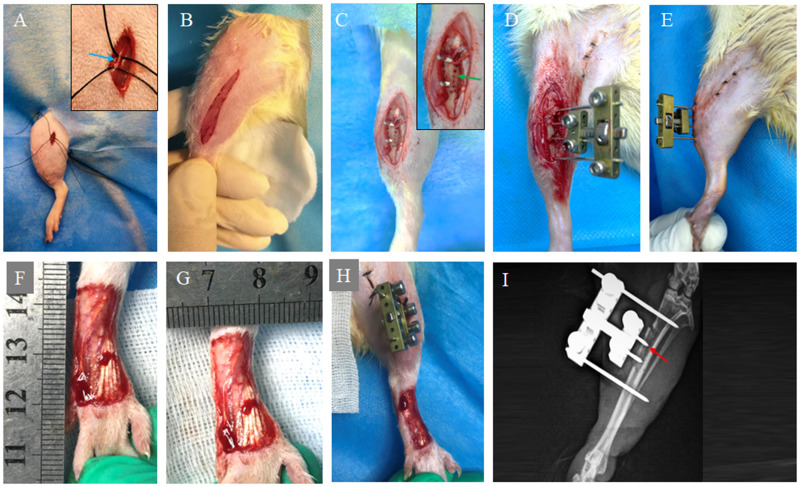
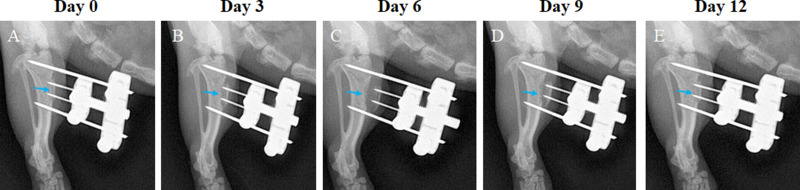
Methods: Severe DFUs were induced in rats, then assigned to TTT, sham, or control groups (n=16/group). The TTT group underwent a tibial corticotomy, with 6 days each of medial and lateral transport; the sham group had a corticotomy without transport. Ulcer healing was assessed through Laser Doppler, CT angiography, histology, and immunohistochemistry. Serum HIF-1α, PDGF-BB, SDF-1, and VEGF levels were measured by ELISA.
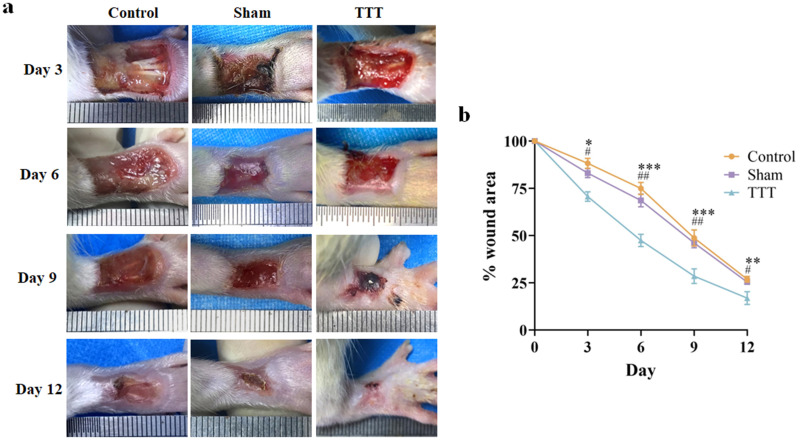
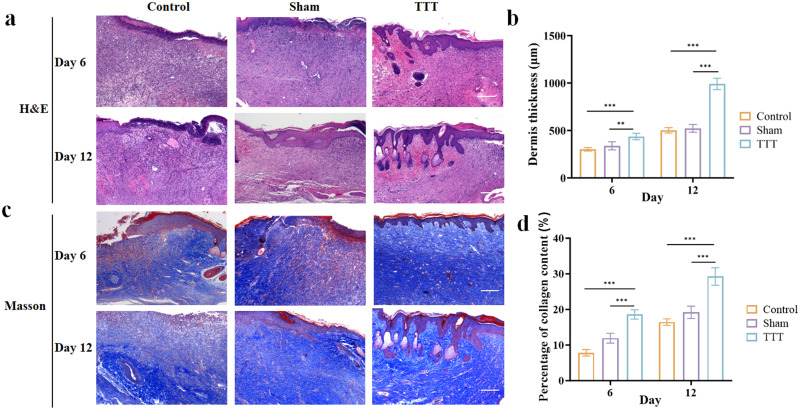
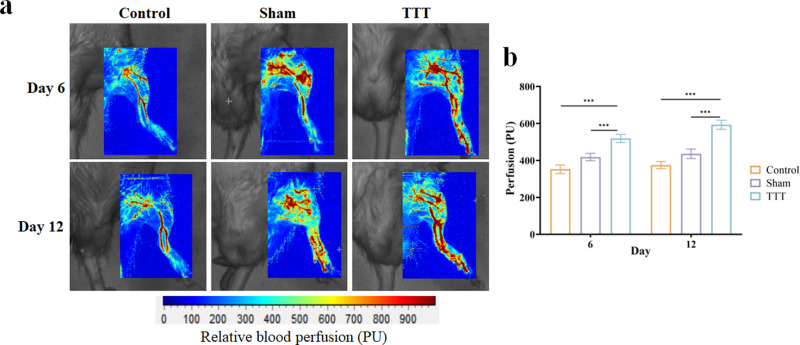
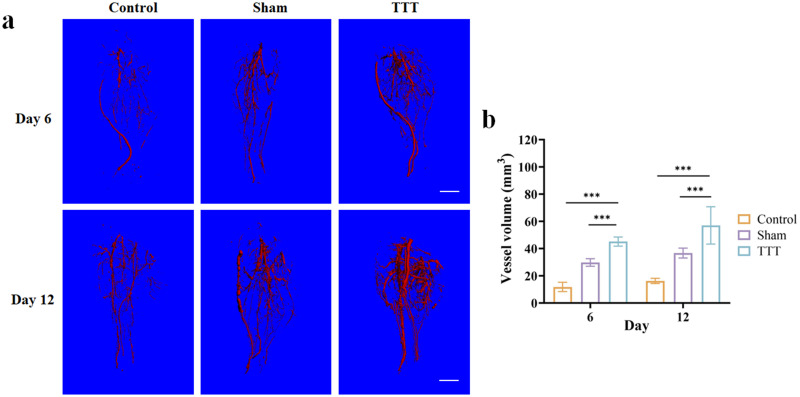
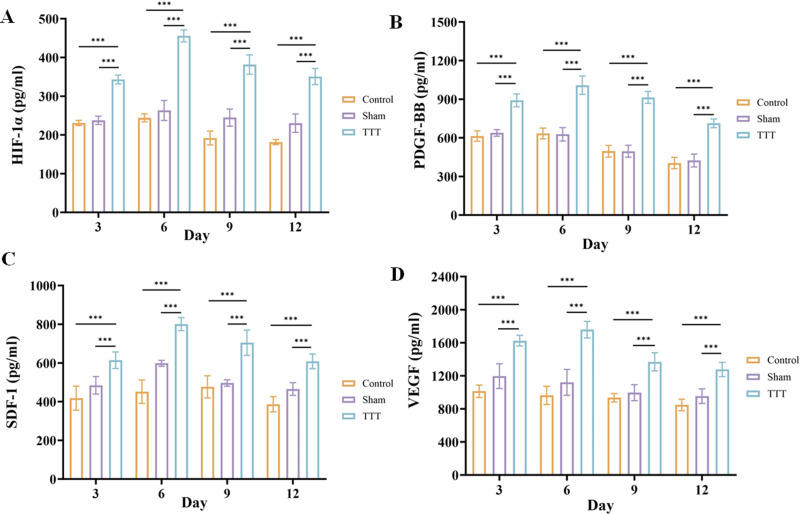
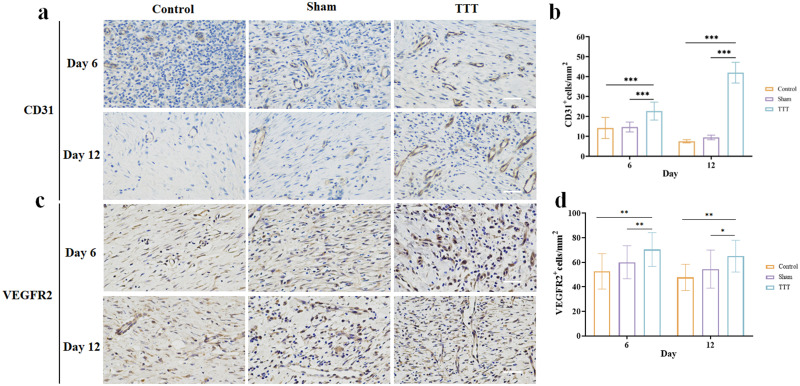
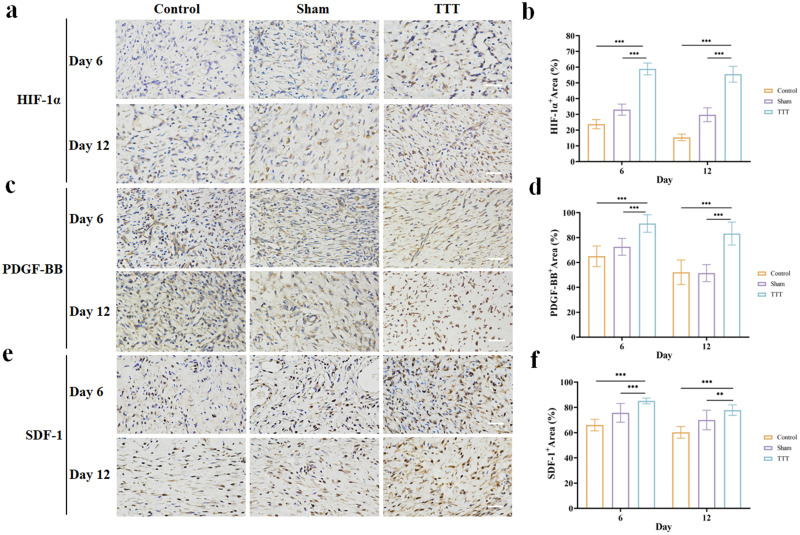
Results: The TTT group showed lower percentages of wound area, higher dermis thickness (all p < 0.001 expect for p = 0.001 for TTT vs Sham at day 6) and percentage of collagen content (all p < 0.001) than the other two groups. The TTT group had higher perfusion and vessel volume in the hindlimb (all p < 0.001). The number of CD31+ cells (all p < 0.001) and VEGFR2+ cells (at day 6, TTT vs Control, p = 0.001, TTT vs Sham, p = 0.006; at day 12, TTT vs Control, p = 0.003, TTT vs Sham, p = 0.01) were higher in the TTT group. The activity of HIF-1α, PDGF-BB, and SDF-1 was increased in the TTT group (all p < 0.001 except for SDF-1 at day 12, TTT vs Sham, p = 0.005). The TTT group had higher levels of HIF-1α, PDGF-BB, SDF-1, and VEGF in serum than the other groups (all p < 0.001).
Conclusion: TTT enhanced neovascularization and perfusion at the hindlimb and accelerated healing of the severe DFUs. The underlying mechanism is related to HIF-1α-induced angiogenesis.
Keywords: HIF-1α; angiogenesis; diabetic foot; distraction osteogenesis; tibial cortex transverse transport.
© 2024 Liu et al.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Tibial cortex transverse transport facilitating healing in patients with recalcitrant non-diabetic leg ulcers.J Orthop Translat. 2020 Dec 9;27:1-7. doi: 10.1016/j.jot.2020.11.001. eCollection 2021 Mar. J Orthop Translat. 2020. PMID: 33344165 Free PMC article.
-
Effect of tibial cortex transverse transport in patients with recalcitrant diabetic foot ulcers: A prospective multicenter cohort study.J Orthop Translat. 2022 Oct 12;36:194-204. doi: 10.1016/j.jot.2022.09.002. eCollection 2022 Sep. J Orthop Translat. 2022. PMID: 36263383 Free PMC article.
-
Triplanar osteotomy combined with proximal tibial transverse transport to accelerate healing of recalcitrant diabetic foot ulcers.J Orthop Surg Res. 2022 Dec 8;17(1):528. doi: 10.1186/s13018-022-03410-z. J Orthop Surg Res. 2022. Retraction in: J Orthop Surg Res. 2023 Nov 17;18(1):874. doi: 10.1186/s13018-023-04351-x PMID: 36482382 Free PMC article. Retracted.
-
[Biological mechanisms of tibial transverse transport for promoting microcirculation and tissue repair].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020 Aug 15;34(8):964-968. doi: 10.7507/1002-1892.202003042. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2020. PMID: 32794662 Free PMC article. Review. Chinese.
-
Disturbed hypoxic responses as a pathogenic mechanism of diabetic foot ulcers.Diabetes Metab Res Rev. 2016 Jan;32 Suppl 1:179-85. doi: 10.1002/dmrr.2742. Diabetes Metab Res Rev. 2016. PMID: 26453314 Review.
Cited by
-
Tibial transverse transport promotes wound healing in diabetic foot ulcers by stimulating endothelial progenitor cell mobilization and homing mediated neovascularization.Ann Med. 2024 Sep 11;56(1):2404186. doi: 10.1080/07853890.2024.2404186. Epub 2024 Sep 16. Ann Med. 2024. PMID: 39283034 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
