

Health Care Utilization and Clinical Management of All-Cause and Norovirus-Associated Acute Gastroenteritis Within a US Integrated Health Care System
- PMID: 38628950
- PMCID: PMC11020278
- DOI: 10.1093/ofid/ofae151
Health Care Utilization and Clinical Management of All-Cause and Norovirus-Associated Acute Gastroenteritis Within a US Integrated Health Care System
Abstract
Background: Norovirus-associated acute gastroenteritis (AGE) exacts a substantial disease burden, yet the health care utilization for and clinical management of norovirus-associated AGE are not well characterized.
Methods: We describe the health care encounters and therapeutics used for patients with all-cause and norovirus-associated AGE in the Kaiser Permanente Northwest health system from 1 April 2014 through 30 September 2016. Medical encounters for patients with AGE were extracted from electronic health records, and encounters within 30 days of one another were grouped into single episodes. An age-stratified random sample of patients completed surveys and provided stool samples for norovirus testing.
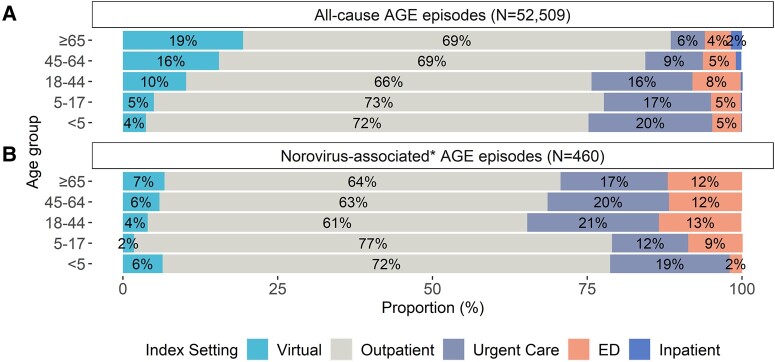
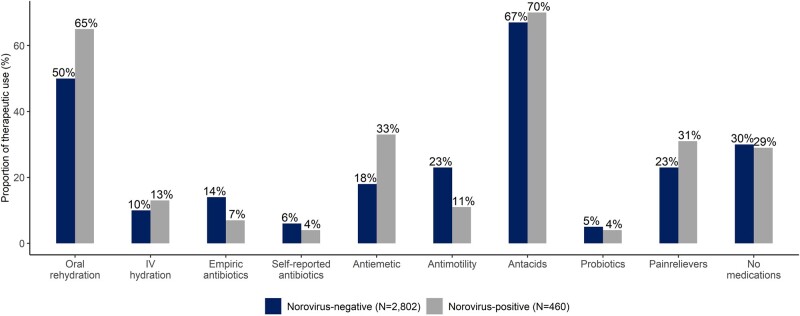
Results: In total, 40 348 individuals had 52 509 AGE episodes; 460 (14%) of 3310 participants in the substudy tested positive for norovirus. An overall 35% of all-cause AGE episodes and 29% of norovirus-associated AGE episodes had ≥2 encounters. While 80% of norovirus-associated AGE episodes had at least 1 encounter in the outpatient setting, all levels of the health care system were affected: 10%, 22%, 10%, and 2% of norovirus-associated AGE episodes had at least 1 encounter in virtual, urgent care, emergency department, and inpatient settings, respectively. Corresponding proportions of therapeutic use between norovirus-positive and norovirus-negative episodes were 13% and 10% for intravenous hydration (P = .07), 65% and 50% for oral rehydration (P < .001), 7% and 14% for empiric antibiotic therapy (P < .001), and 33% and 18% for antiemetics (P < .001).
Conclusions: Increased health care utilization and therapeutics are likely needed for norovirus-associated AGE episodes during peak norovirus winter seasons, and these data illustrate that effective norovirus vaccines will likely result in less health care utilization.
Keywords: acute gastroenteritis; clinical management; diarrhea; health care utilization; norovirus.
Published by Oxford University Press on behalf of Infectious Diseases Society of America 2024.
Conflict of interest statement
Potential conflicts of interest. A. L. N. has received research funding from Pfizer, Merck, and MedImmune (now AstraZeneca) for unrelated studies. All other authors report no potential conflicts.
Figures
Similar articles
-
Norovirus and Other Viral Causes of Medically Attended Acute Gastroenteritis Across the Age Spectrum: Results from the Medically Attended Acute Gastroenteritis Study in the United States.Clin Infect Dis. 2021 Aug 16;73(4):e913-e920. doi: 10.1093/cid/ciab033. Clin Infect Dis. 2021. PMID: 34398953 Free PMC article.
-
Incidence of Norovirus and Other Viral Pathogens That Cause Acute Gastroenteritis (AGE) among Kaiser Permanente Member Populations in the United States, 2012-2013.PLoS One. 2016 Apr 26;11(4):e0148395. doi: 10.1371/journal.pone.0148395. eCollection 2016. PLoS One. 2016. PMID: 27115485 Free PMC article.
-
Trends in Incidence of Norovirus-associated Acute Gastroenteritis in 4 Veterans Affairs Medical Center Populations in the United States, 2011-2015.Clin Infect Dis. 2020 Jan 1;70(1):40-48. doi: 10.1093/cid/ciz165. Clin Infect Dis. 2020. PMID: 30901024 Free PMC article.
-
The Vast and Varied Global Burden of Norovirus: Prospects for Prevention and Control.PLoS Med. 2016 Apr 26;13(4):e1001999. doi: 10.1371/journal.pmed.1001999. eCollection 2016 Apr. PLoS Med. 2016. PMID: 27115709 Free PMC article. Review.
-
Global prevalence of norovirus in cases of gastroenteritis: a systematic review and meta-analysis.Lancet Infect Dis. 2014 Aug;14(8):725-730. doi: 10.1016/S1473-3099(14)70767-4. Epub 2014 Jun 26. Lancet Infect Dis. 2014. PMID: 24981041 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
