

Reducing Hospitalizations and Multidrug-Resistant Organisms via Regional Decolonization in Hospitals and Nursing Homes
- PMID: 38557703
- PMCID: PMC10985619
- DOI: 10.1001/jama.2024.2759
Reducing Hospitalizations and Multidrug-Resistant Organisms via Regional Decolonization in Hospitals and Nursing Homes
Abstract
Importance: Infections due to multidrug-resistant organisms (MDROs) are associated with increased morbidity, mortality, length of hospitalization, and health care costs. Regional interventions may be advantageous in mitigating MDROs and associated infections.
Objective: To evaluate whether implementation of a decolonization collaborative is associated with reduced regional MDRO prevalence, incident clinical cultures, infection-related hospitalizations, costs, and deaths.
Design, setting, and participants: This quality improvement study was conducted from July 1, 2017, to July 31, 2019, across 35 health care facilities in Orange County, California.
Exposures: Chlorhexidine bathing and nasal iodophor antisepsis for residents in long-term care and hospitalized patients in contact precautions (CP).
Main outcomes and measures: Baseline and end of intervention MDRO point prevalence among participating facilities; incident MDRO (nonscreening) clinical cultures among participating and nonparticipating facilities; and infection-related hospitalizations and associated costs and deaths among residents in participating and nonparticipating nursing homes (NHs).
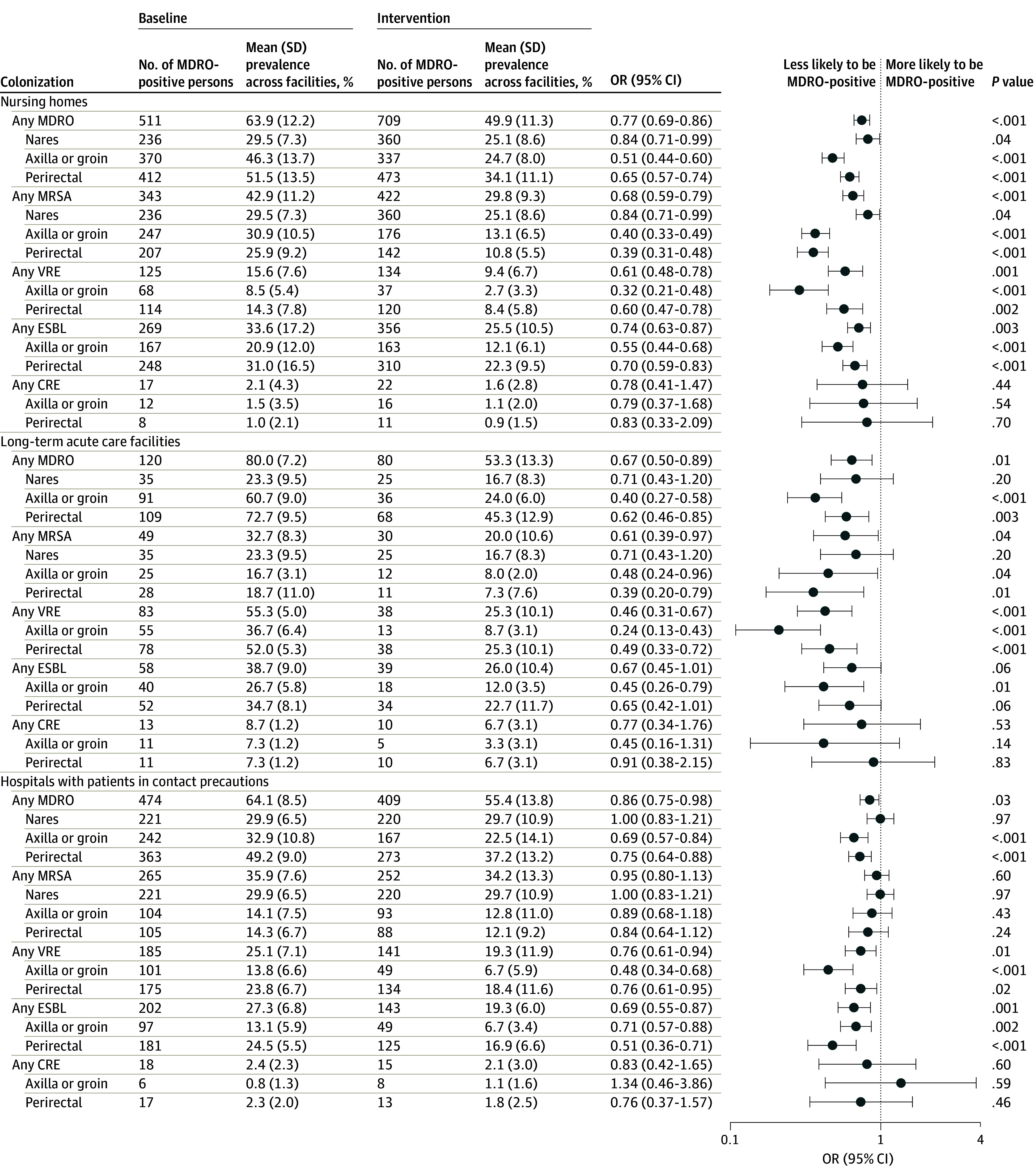
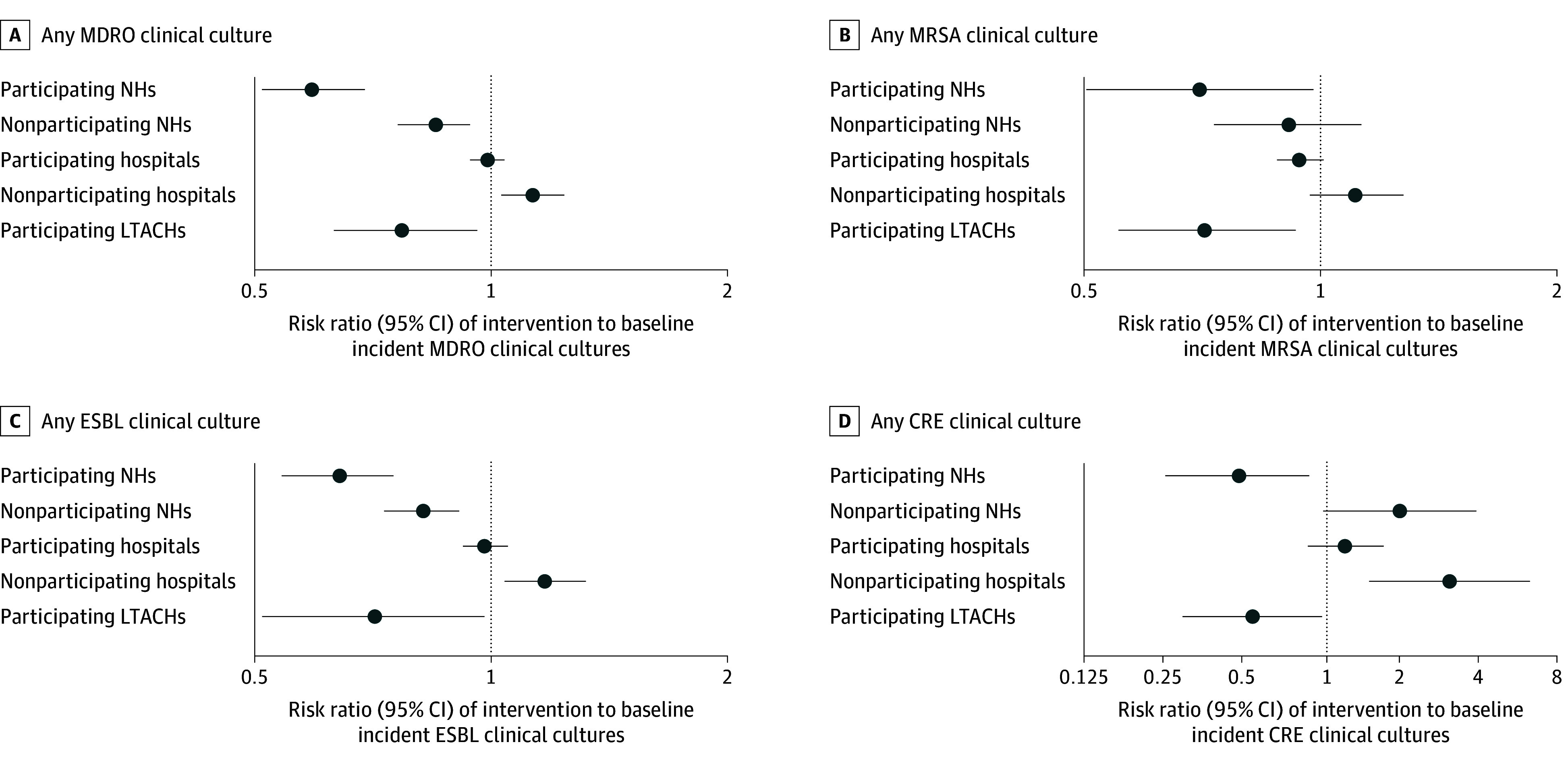
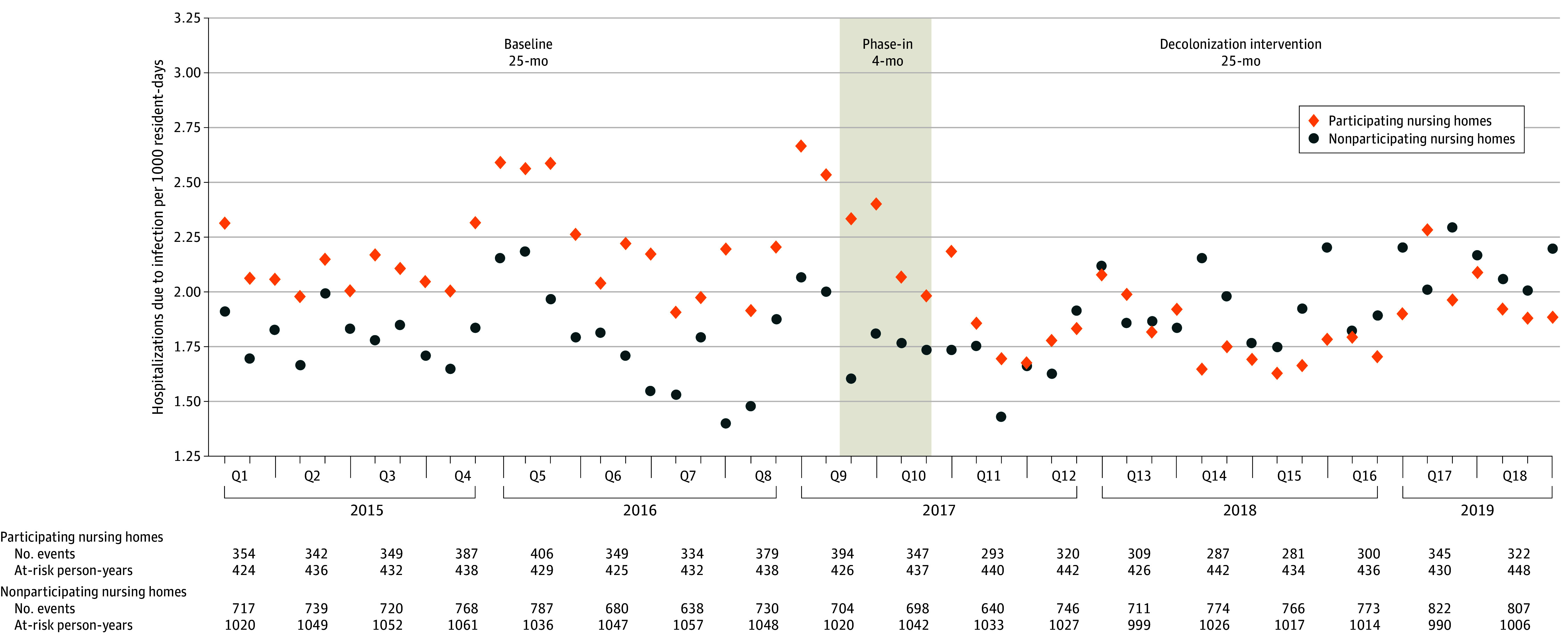
Results: Thirty-five facilities (16 hospitals, 16 NHs, 3 long-term acute care hospitals [LTACHs]) adopted the intervention. Comparing decolonization with baseline periods among participating facilities, the mean (SD) MDRO prevalence decreased from 63.9% (12.2%) to 49.9% (11.3%) among NHs, from 80.0% (7.2%) to 53.3% (13.3%) among LTACHs (odds ratio [OR] for NHs and LTACHs, 0.48; 95% CI, 0.40-0.57), and from 64.1% (8.5%) to 55.4% (13.8%) (OR, 0.75; 95% CI, 0.60-0.93) among hospitalized patients in CP. When comparing decolonization with baseline among NHs, the mean (SD) monthly incident MDRO clinical cultures changed from 2.7 (1.9) to 1.7 (1.1) among participating NHs, from 1.7 (1.4) to 1.5 (1.1) among nonparticipating NHs (group × period interaction reduction, 30.4%; 95% CI, 16.4%-42.1%), from 25.5 (18.6) to 25.0 (15.9) among participating hospitals, from 12.5 (10.1) to 14.3 (10.2) among nonparticipating hospitals (group × period interaction reduction, 12.9%; 95% CI, 3.3%-21.5%), and from 14.8 (8.6) to 8.2 (6.1) among LTACHs (all facilities participating; 22.5% reduction; 95% CI, 4.4%-37.1%). For NHs, the rate of infection-related hospitalizations per 1000 resident-days changed from 2.31 during baseline to 1.94 during intervention among participating NHs, and from 1.90 to 2.03 among nonparticipating NHs (group × period interaction reduction, 26.7%; 95% CI, 19.0%-34.5%). Associated hospitalization costs per 1000 resident-days changed from $64 651 to $55 149 among participating NHs and from $55 151 to $59 327 among nonparticipating NHs (group × period interaction reduction, 26.8%; 95% CI, 26.7%-26.9%). Associated hospitalization deaths per 1000 resident-days changed from 0.29 to 0.25 among participating NHs and from 0.23 to 0.24 among nonparticipating NHs (group × period interaction reduction, 23.7%; 95% CI, 4.5%-43.0%).
Conclusions and relevance: A regional collaborative involving universal decolonization in long-term care facilities and targeted decolonization among hospital patients in CP was associated with lower MDRO carriage, infections, hospitalizations, costs, and deaths.
Conflict of interest statement
Figures
Comment in
-
Controlling Multidrug-Resistant Organisms Across Patient-Sharing Networks.JAMA. 2024 May 14;331(18):1532-1533. doi: 10.1001/jama.2024.0267. JAMA. 2024. PMID: 38557704 No abstract available.
Similar articles
-
Controlling Multidrug-Resistant Organisms Across Patient-Sharing Networks.JAMA. 2024 May 14;331(18):1532-1533. doi: 10.1001/jama.2024.0267. JAMA. 2024. PMID: 38557704 No abstract available.
-
Effectiveness of a Multicomponent Intervention to Reduce Multidrug-Resistant Organisms in Nursing Homes: A Cluster Randomized Clinical Trial.JAMA Netw Open. 2021 Jul 1;4(7):e2116555. doi: 10.1001/jamanetworkopen.2021.16555. JAMA Netw Open. 2021. PMID: 34269807 Free PMC article. Clinical Trial.
-
The SHIELD Orange County Project: Multidrug-resistant Organism Prevalence in 21 Nursing Homes and Long-term Acute Care Facilities in Southern California.Clin Infect Dis. 2019 Oct 15;69(9):1566-1573. doi: 10.1093/cid/ciz119. Clin Infect Dis. 2019. PMID: 30753383 Free PMC article.
-
An integrative review of infection prevention and control programs for multidrug-resistant organisms in acute care hospitals: a socio-ecological perspective.Am J Infect Control. 2011 Jun;39(5):368-378. doi: 10.1016/j.ajic.2010.07.017. Epub 2011 Mar 23. Am J Infect Control. 2011. PMID: 21429622 Review.
-
[Effect of 2% Chlorhexidine Bathing on the Incidence of Hospital-Acquired Infection and Multidrug-Resistant Organisms in Adult Intensive Care Unit Patients: Systematic Review and Meta-Analysis].J Korean Acad Nurs. 2021 Aug;51(4):414-429. doi: 10.4040/jkan.21046. J Korean Acad Nurs. 2021. PMID: 34497251 Review. Korean.
Cited by
-
Intertwining clonality and resistance: Staphylococcus aureus in the antibiotic era.J Clin Invest. 2024 Oct 1;134(19):e185824. doi: 10.1172/JCI185824. J Clin Invest. 2024. PMID: 39352382 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention . Antibiotic Resistance Threats in the United States. Department of Health and Human Services; 2019.
-
- World Health Organization . Ten threats to global health in 2019. Published 2019. Accessed October 31, 2023. https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
