

Glioblastoma Therapy: Past, Present and Future
- PMID: 38473776
- PMCID: PMC10931797
- DOI: 10.3390/ijms25052529
Glioblastoma Therapy: Past, Present and Future
Abstract
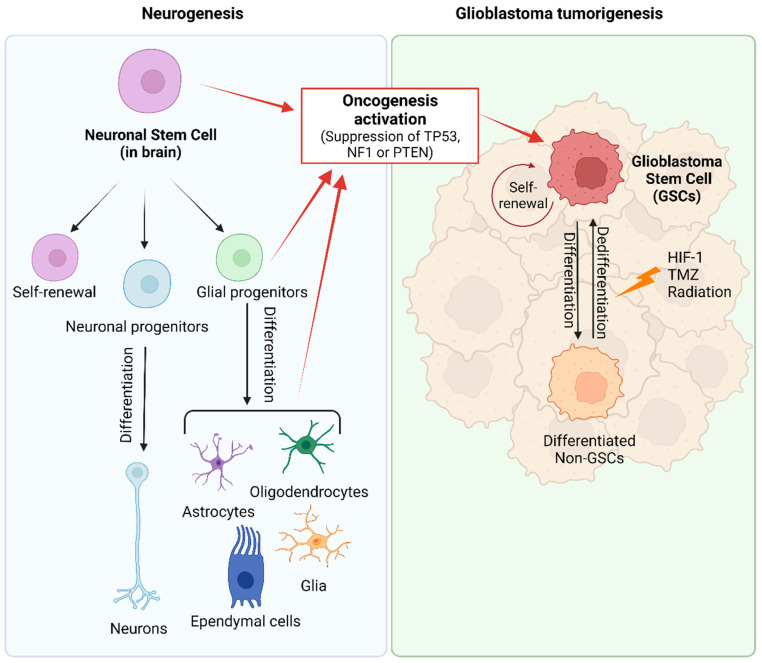
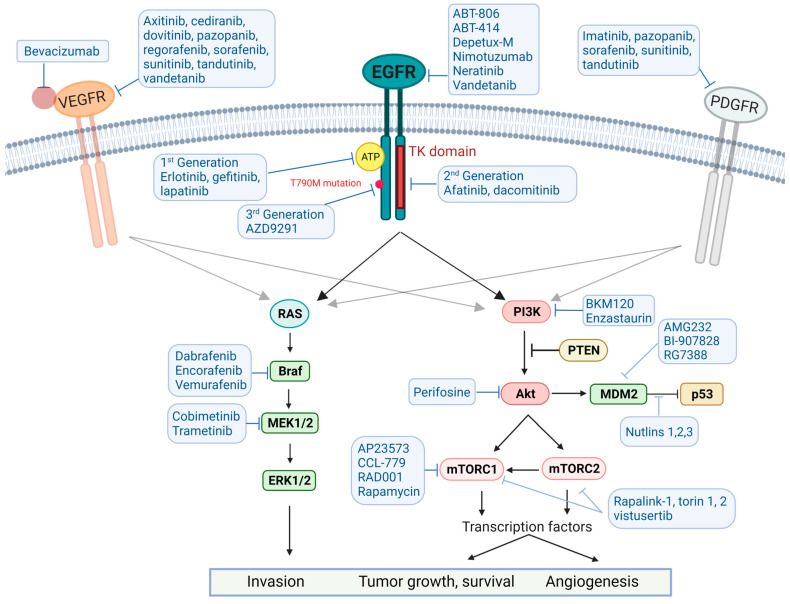
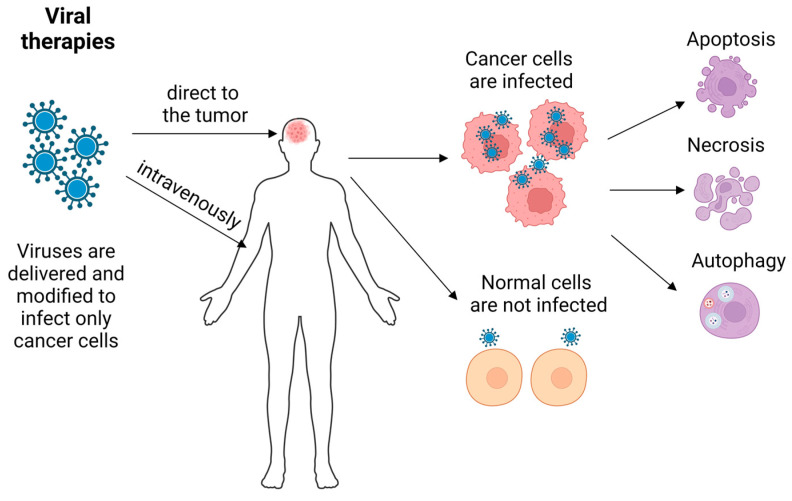
Glioblastoma (GB) stands out as the most prevalent and lethal form of brain cancer. Although great efforts have been made by clinicians and researchers, no significant improvement in survival has been achieved since the Stupp protocol became the standard of care (SOC) in 2005. Despite multimodality treatments, recurrence is almost universal with survival rates under 2 years after diagnosis. Here, we discuss the recent progress in our understanding of GB pathophysiology, in particular, the importance of glioma stem cells (GSCs), the tumor microenvironment conditions, and epigenetic mechanisms involved in GB growth, aggressiveness and recurrence. The discussion on therapeutic strategies first covers the SOC treatment and targeted therapies that have been shown to interfere with different signaling pathways (pRB/CDK4/RB1/P16ink4, TP53/MDM2/P14arf, PI3k/Akt-PTEN, RAS/RAF/MEK, PARP) involved in GB tumorigenesis, pathophysiology, and treatment resistance acquisition. Below, we analyze several immunotherapeutic approaches (i.e., checkpoint inhibitors, vaccines, CAR-modified NK or T cells, oncolytic virotherapy) that have been used in an attempt to enhance the immune response against GB, and thereby avoid recidivism or increase survival of GB patients. Finally, we present treatment attempts made using nanotherapies (nanometric structures having active anti-GB agents such as antibodies, chemotherapeutic/anti-angiogenic drugs or sensitizers, radionuclides, and molecules that target GB cellular receptors or open the blood-brain barrier) and non-ionizing energies (laser interstitial thermal therapy, high/low intensity focused ultrasounds, photodynamic/sonodynamic therapies and electroporation). The aim of this review is to discuss the advances and limitations of the current therapies and to present novel approaches that are under development or following clinical trials.
Keywords: glioblastoma; immunotherapy; nanotherapy; non-ionizing radiation; targeted therapy.
Conflict of interest statement
Authors Elena Obrador, Paz Moreno-Murciano, María Oriol-Caballo, Rafael López-Blanch and José M. Estrela were employed by Scientia BioTech S.L. The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Combinatorial approaches to effective therapy in glioblastoma (GBM): Current status and what the future holds.Int Rev Immunol. 2022;41(6):582-605. doi: 10.1080/08830185.2022.2101647. Epub 2022 Aug 8. Int Rev Immunol. 2022. PMID: 35938932 Review.
-
Novel Therapies in Glioblastoma Treatment: Review of Glioblastoma; Current Treatment Options; and Novel Oncolytic Viral Therapies.Med Sci (Basel). 2023 Dec 23;12(1):1. doi: 10.3390/medsci12010001. Med Sci (Basel). 2023. PMID: 38249077 Free PMC article. Review.
-
Present and potential future adjuvant issues in high-grade astrocytic glioma treatment.Adv Tech Stand Neurosurg. 2009;34:3-35. doi: 10.1007/978-3-211-78741-0_1. Adv Tech Stand Neurosurg. 2009. PMID: 19368079 Review.
-
Oncolytic herpes simplex viruses for the treatment of glioma and targeting glioblastoma stem-like cells.Front Cell Infect Microbiol. 2023 May 31;13:1206111. doi: 10.3389/fcimb.2023.1206111. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37325516 Free PMC article. Review.
-
Oncolytic Viruses for Malignant Glioma: On the Verge of Success?Viruses. 2021 Jul 2;13(7):1294. doi: 10.3390/v13071294. Viruses. 2021. PMID: 34372501 Free PMC article. Review.
Cited by
-
The Importance of Biotinylation for the Suitability of Cationic and Neutral Fourth-Generation Polyamidoamine Dendrimers as Targeted Drug Carriers in the Therapy of Glioma and Liver Cancer.Molecules. 2024 Sep 10;29(18):4293. doi: 10.3390/molecules29184293. Molecules. 2024. PMID: 39339289 Free PMC article.
-
Adipose-Derived Stem Cells as Carrier of Pro-Apoptotic Oncolytic Myxoma Virus: To Cross the Blood-Brain Barrier and Treat Murine Glioma.Int J Mol Sci. 2024 Oct 18;25(20):11225. doi: 10.3390/ijms252011225. Int J Mol Sci. 2024. PMID: 39457007 Free PMC article.
-
Prospects of marine-derived compounds as potential therapeutic agents for glioma.Pharm Biol. 2024 Dec;62(1):513-526. doi: 10.1080/13880209.2024.2359659. Epub 2024 Jun 12. Pharm Biol. 2024. PMID: 38864445 Free PMC article. Review.
-
Recent Treatment Strategies and Molecular Pathways in Resistance Mechanisms of Antiangiogenic Therapies in Glioblastoma.Cancers (Basel). 2024 Aug 27;16(17):2975. doi: 10.3390/cancers16172975. Cancers (Basel). 2024. PMID: 39272834 Free PMC article. Review.
-
Understanding the Significance of Hypoxia-Inducible Factors (HIFs) in Glioblastoma: A Systematic Review.Cancers (Basel). 2024 May 30;16(11):2089. doi: 10.3390/cancers16112089. Cancers (Basel). 2024. PMID: 38893207 Free PMC article. Review.
References
-
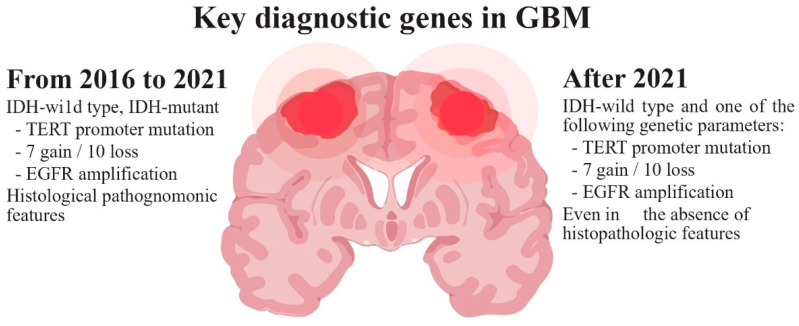
- Louis D.N., Perry A., Wesseling P., Brat D.J., Cree I.A., Figarella-Branger D., Hawkins C., Ng H.K., Pfister S.M., Reifenberger G., et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncology. 2021;23:1231–1251. doi: 10.1093/neuonc/noab106. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
