

Health Canada advisory impacts on the prevalence of oral codeine use in the Pediatric Canadian population: comparative study across provinces
- PMID: 38438444
- PMCID: PMC10912710
- DOI: 10.1038/s41598-024-55758-3
Health Canada advisory impacts on the prevalence of oral codeine use in the Pediatric Canadian population: comparative study across provinces
Abstract
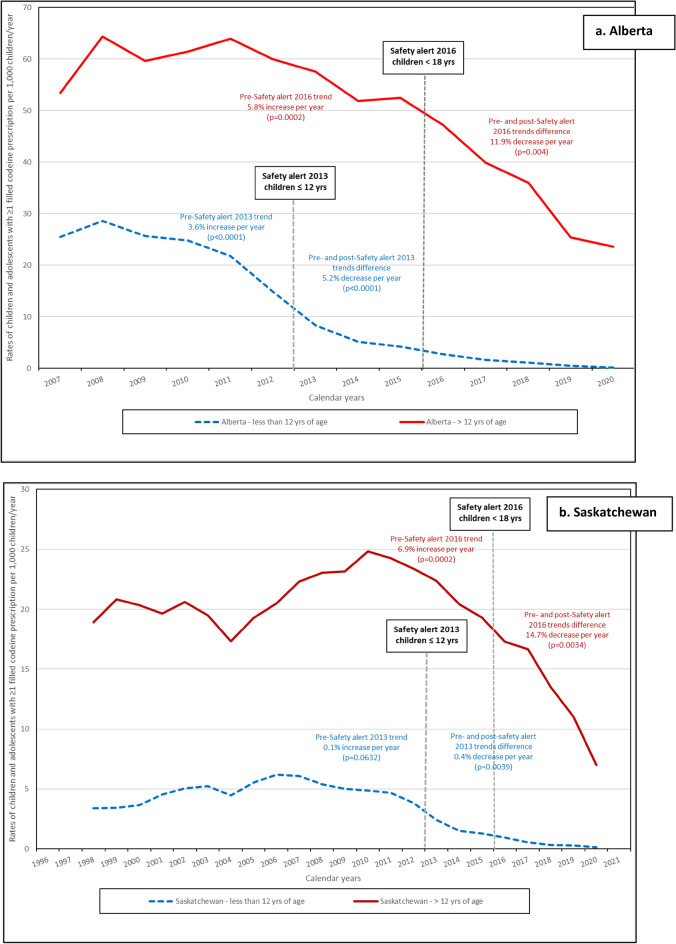
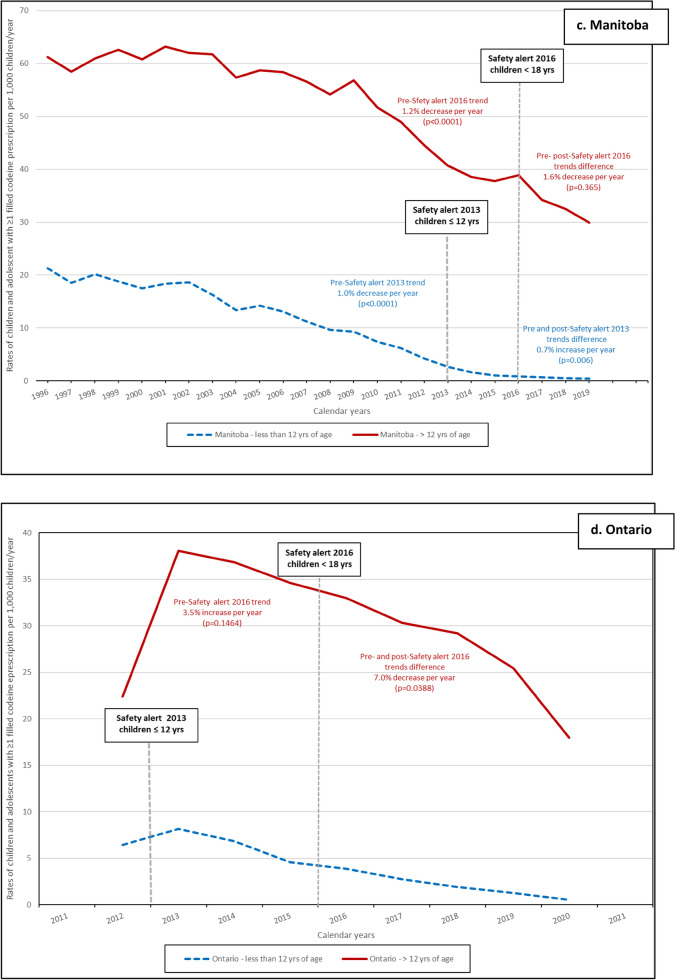
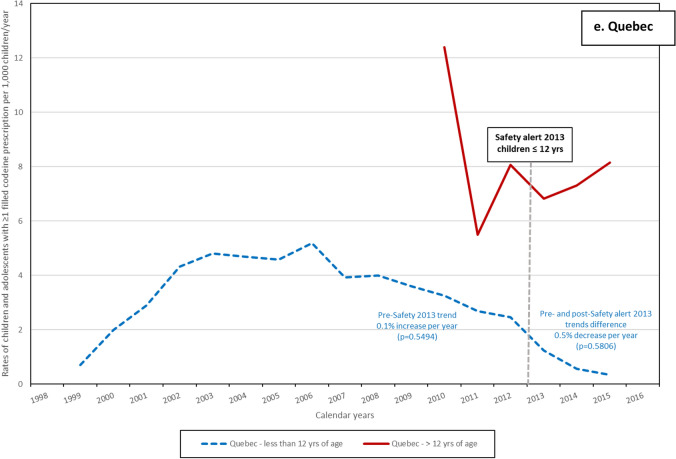
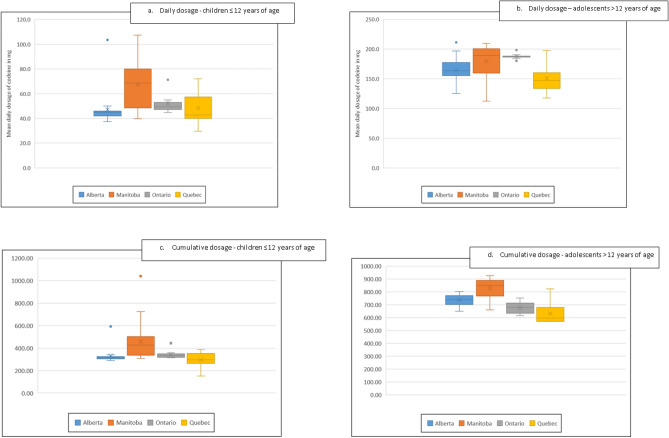
Health Canada (HC) has, since 2013, issued safety alerts restricting the use of codeine-containing drugs among breastfeeding women and children/adolescents under 18 years of age. These products are linked to breathing problems among ultra-rapid CYP2D6 metabolizers and early use of opioid can lead to future opioid misuse. Using a multi-province population-based cohort study, we estimate the impact of federal safety alerts on annual rates of codeine use in the Canadian pediatric population. We analyzed data from 8,156,948 children/adolescents in five Canadian provinces between 1996 and 2021, using a common protocol. Children/adolescents were categorized as: ≤ 12 years (children) or > 12 years (adolescents). We defined codeine exposure by ≥ 1 prescription filled for codeine alone or combined with other medications. For both age categories, we obtained province-specific codeine prescription filling rates per calendar year by dividing the number of children/adolescents with ≥ 1 codeine prescription filled by the number of person-time. Annual rates of codeine use per 1000 persons vary by province from 3.0 (Quebec) to 10.1 (Manitoba) in children, and from 5.5 to 51.3 in adolescents. After the 2013 HC advisory, exposure decreased in all provinces (adjusted level change from - 0.6 to - 18.4%) in children and from - 2.1 to - 17.9% in adolescents after the 2016 advisory. Annual rates declined over time in all provinces, following HC safety alerts specific to each of the two age categories.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The impact of proposed regulatory changes and rescheduling on low-dose codeine purchasing in Canada: a time-series analysis.CMAJ Open. 2021 Dec 14;9(4):E1181-E1186. doi: 10.9778/cmajo.20210173. Print 2021 Oct-Dec. CMAJ Open. 2021. PMID: 34906994 Free PMC article.
-
Prescription opioid dispensing in Australian children and adolescents: a national population-based study.Lancet Child Adolesc Health. 2019 Dec;3(12):881-888. doi: 10.1016/S2352-4642(19)30329-3. Epub 2019 Oct 8. Lancet Child Adolesc Health. 2019. PMID: 31604614
-
Medications Containing Low-Dose Codeine for the Treatment of Pain and Coughs [Internet].Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2021 Aug. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2021 Aug. PMID: 36279380 Free Books & Documents. Review.
-
Correlations between opioid mortality increases related to illicit/synthetic opioids and reductions of medical opioid dispensing - exploratory analyses from Canada.BMC Public Health. 2020 Jan 31;20(1):143. doi: 10.1186/s12889-020-8205-z. BMC Public Health. 2020. PMID: 32005211 Free PMC article.
-
Codeine and opioid metabolism: implications and alternatives for pediatric pain management.Curr Opin Anaesthesiol. 2017 Jun;30(3):349-356. doi: 10.1097/ACO.0000000000000455. Curr Opin Anaesthesiol. 2017. PMID: 28323671 Free PMC article. Review.
References
-
- Chua, K. P., Shrime, M. G. & Conti, R. M. Effect of FDA investigation on opioid prescribing to children after tonsillectomy/adenoidectomy. Pediatrics140(6) (2017). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
