

Value of carotid intima thickness in assessing advanced carotid plaque vulnerability: a study based on carotid artery ultrasonography and carotid plaque histology
- PMID: 38415155
- PMCID: PMC10895139
- DOI: 10.21037/qims-23-1193
Value of carotid intima thickness in assessing advanced carotid plaque vulnerability: a study based on carotid artery ultrasonography and carotid plaque histology
Abstract
Background: Research has shown that carotid intima-media thickness (CIMT) could help to predict carotid plaque (CP) progression in patients with mild carotid stenosis. However, the debate continues as to the value of carotid intima thickness (CIT) in monitoring the development of CP in patients with severe carotid stenosis. This study sought to evaluate the relationships between CIT and the ultrasonic characteristics of CP and to analyze the value of CIT and the ultrasonic parameters of CP in assessing plaque vulnerability in advanced human carotid atherosclerosis.
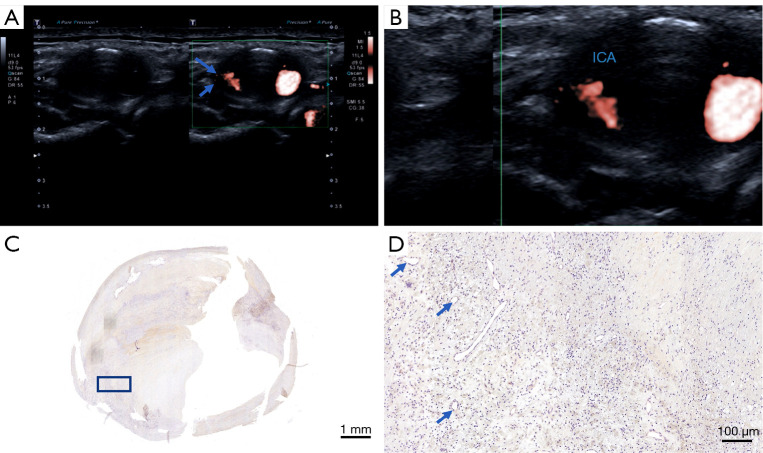
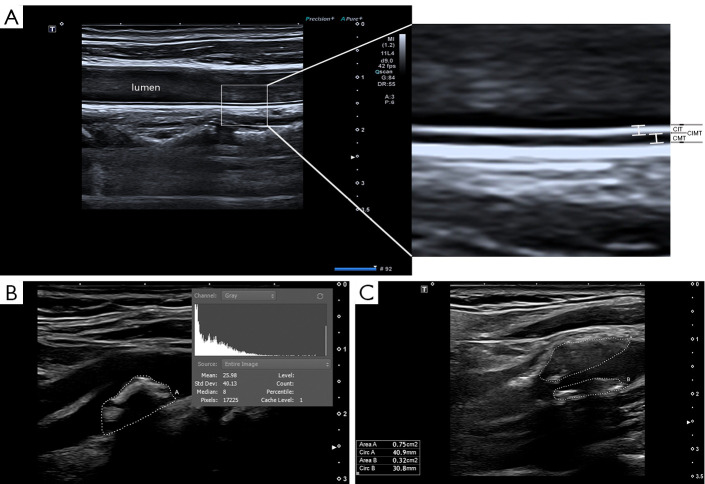
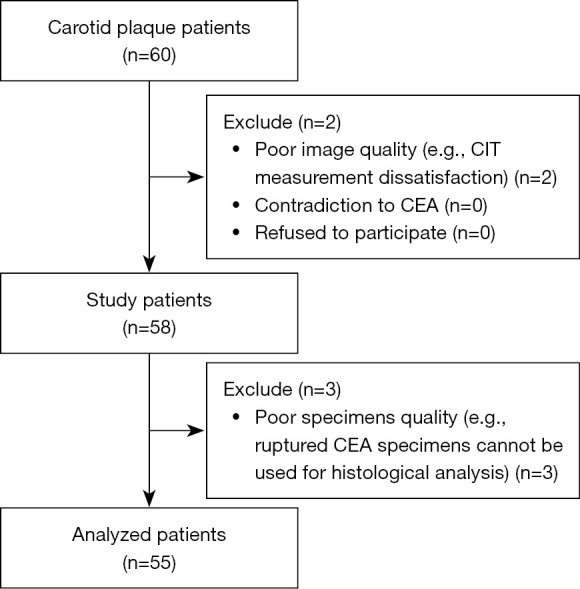
Methods: A total of 55 individuals who underwent carotid endarterectomy (CEA) were included in the study (mean age: 65±7 years; female: 9.1%). CIMT and CIT were examined at the common carotid artery (CCA). Plaque textural features, such as the gray-scale median (GSM), superb microvascular imaging (SMI) level, and total plaque area (TPA), were also identified. A Spearman correlation coefficient analysis was performed to examine the relationship between CIT and the ultrasonic parameters of CP. The CIT of various plaque types was compared. Receiver operating characteristic (ROC) curves were used to analyze the diagnostic values of the ultrasound characteristics to evaluate CP vulnerability.
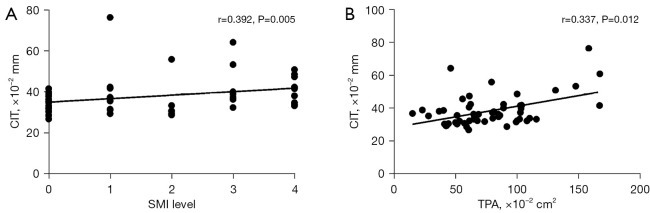
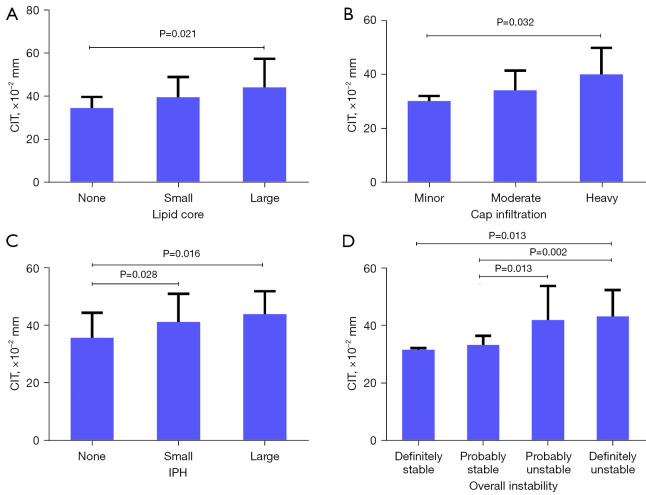
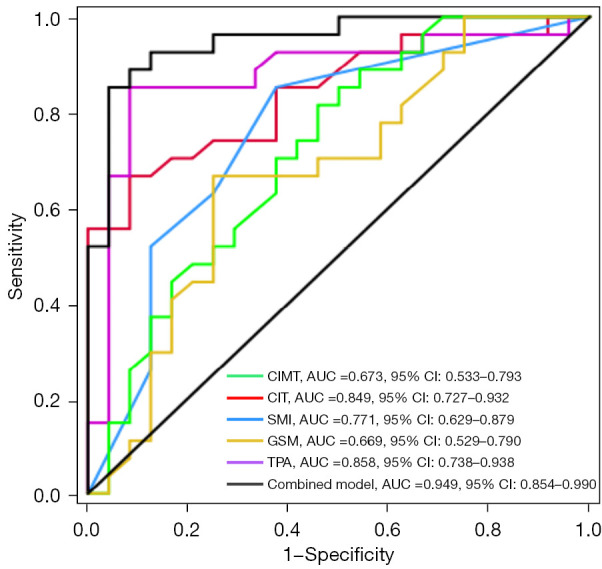
Results: The mean CIT of all the participants was 0.382±0.095 mm, the mean CIT of the participants with stable plaques was 0.328±0.031 mm, and the mean CIT of participants with vulnerable plaques was 0.424±0.106 mm (P<0.001). CIT was associated with the SMI level (Spearman's correlation coefficient: r=0.392, P=0.005), TPA (Spearman's correlation coefficient: r=0.337, P=0.012). Patients with thicker CIT had larger lipid cores, higher levels of plaque vulnerability, and more intraplaque hemorrhages (IPHs). The areas under the ROCs (AUCs) with 95% confidence interval (CI) for CIMT, CIT, the SMI level, the GSM, the TPA, and the combined model for identifying vulnerable plaques were 0.673 (0.533-0.793), 0.849 (0.727-0.932), 0.771 (0.629-0.879), 0.669 (0.529-0.790), 0.858 (0.738-0.938), and 0.949 (0.854-0.990), respectively.
Conclusions: CIT was associated with both the histology and ultrasonic features of CP. CIT may be helpful in the detection of severe CP development.
Keywords: Carotid intima thickness (CIT); gray-scale median (GSM); plaque vulnerability; superb microvascular imaging (SMI); total plaque area (TPA).
2024 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-23-1193/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Common carotid intima-media features determine distal disease phenotype and vulnerability in asymptomatic patients.Int J Cardiol. 2015 Oct 1;196:22-8. doi: 10.1016/j.ijcard.2015.05.168. Epub 2015 Jun 3. Int J Cardiol. 2015. PMID: 26070179
-
Assessment of neovascularization of carotid artery atherosclerotic plaques using superb microvascular imaging: a comparison with contrast-enhanced ultrasound imaging and histology.Quant Imaging Med Surg. 2021 May;11(5):1958-1969. doi: 10.21037/qims-20-933. Quant Imaging Med Surg. 2021. PMID: 33936978 Free PMC article.
-
Cross-sectional analysis of the association of periodontitis with carotid intima media thickness and atherosclerotic plaque in the Hamburg City health study.J Periodontal Res. 2022 Aug;57(4):824-834. doi: 10.1111/jre.13021. Epub 2022 Jun 8. J Periodontal Res. 2022. PMID: 35675038
-
Carotid intima-media thickness and plaque in cardiovascular risk assessment.JACC Cardiovasc Imaging. 2014 Oct;7(10):1025-38. doi: 10.1016/j.jcmg.2013.11.014. Epub 2014 Jul 16. JACC Cardiovasc Imaging. 2014. PMID: 25051948 Review.
-
Contemporary carotid imaging: from degree of stenosis to plaque vulnerability.J Neurosurg. 2016 Jan;124(1):27-42. doi: 10.3171/2015.1.JNS142452. Epub 2015 Jul 31. J Neurosurg. 2016. PMID: 26230478 Review.
Cited by
-
A Non-Coronary, Peripheral Arterial Atherosclerotic Disease (Carotid, Renal, Lower Limb) in Elderly Patients-A Review: Part I-Epidemiology, Risk Factors, and Atherosclerosis-Related Diversities in Elderly Patients.J Clin Med. 2024 Mar 3;13(5):1471. doi: 10.3390/jcm13051471. J Clin Med. 2024. PMID: 38592280 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous