

Characterising polymyalgia rheumatica on whole-body 18F-FDG PET/CT: an atlas
- PMID: 38375531
- PMCID: PMC10876394
- DOI: 10.1093/rap/rkae003
Characterising polymyalgia rheumatica on whole-body 18F-FDG PET/CT: an atlas
Abstract
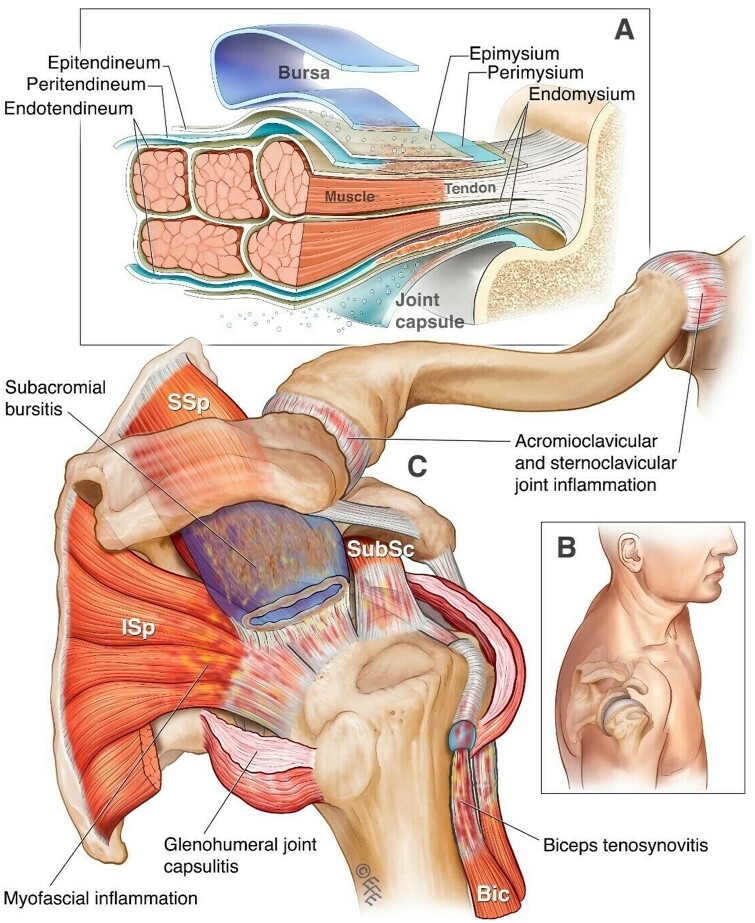
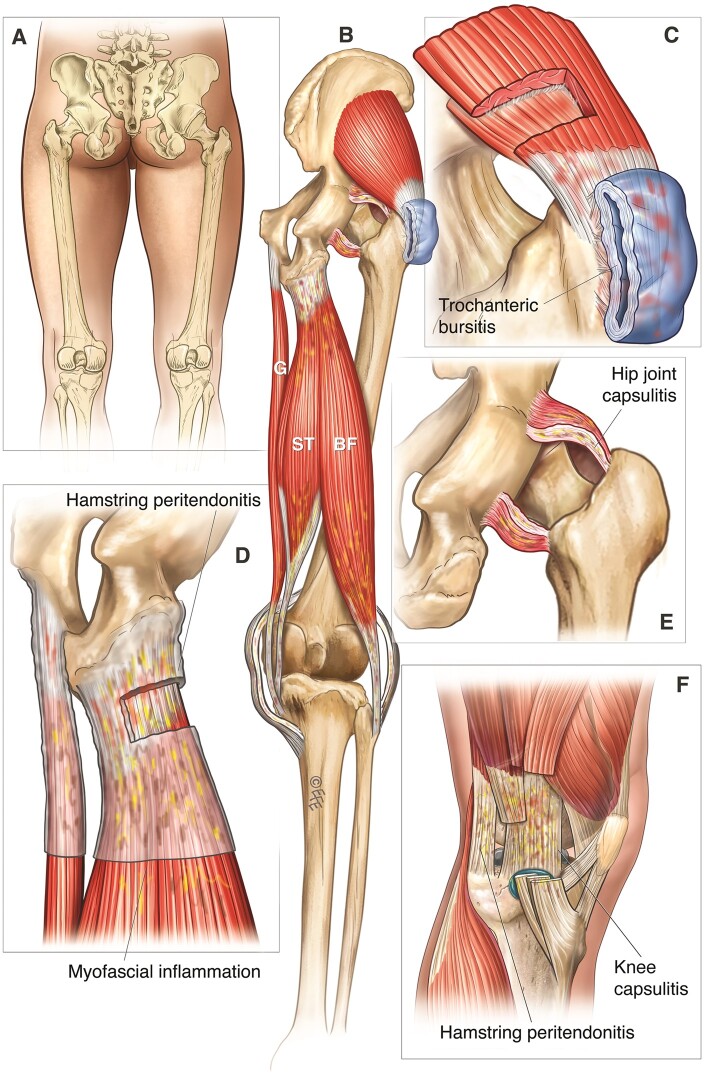
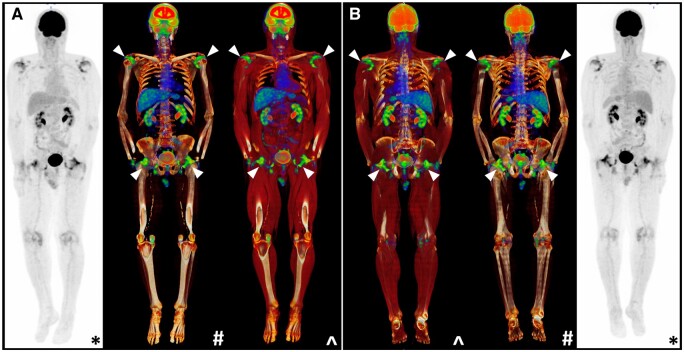
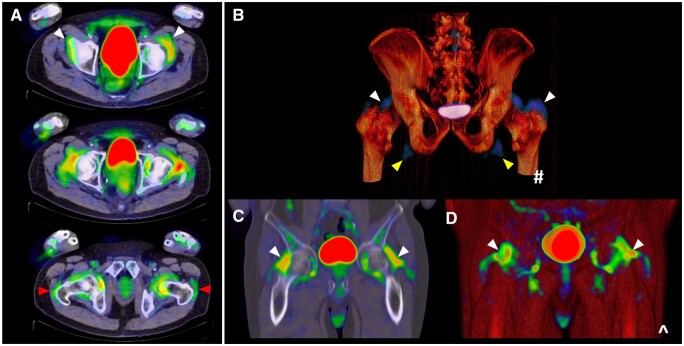
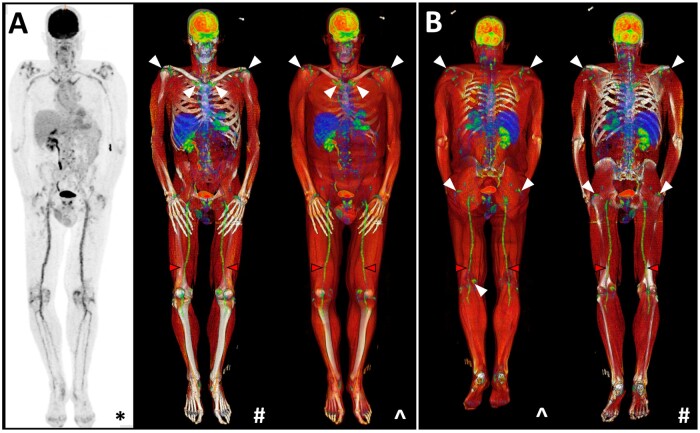
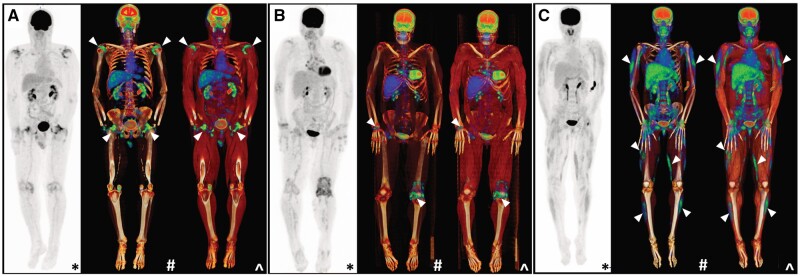
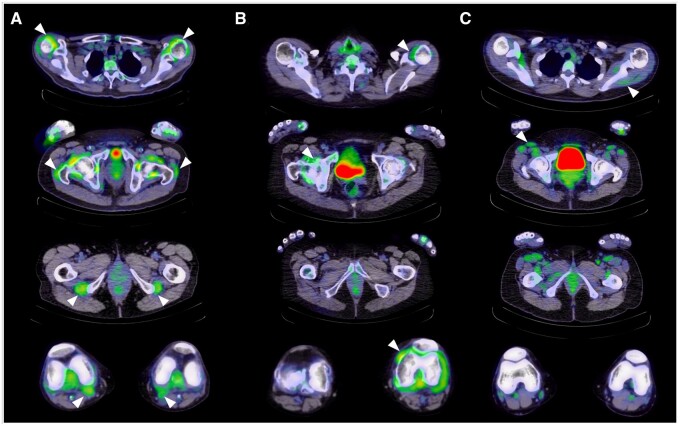
The impact of modern imaging in uncovering the underlying pathology of PMR cannot be understated. Long dismissed as an inflammatory syndrome with links to the large vessel vasculitis giant cell arteritis (GCA), a pathognomonic pattern of musculotendinous inflammation is now attributed to PMR and may be used to confirm its diagnosis. Among the available modalities, 18F-fluorodeoxyglucose (18F-FDG) PET/CT is increasingly recognized for its high sensitivity and specificity, as well as added ability to detect concomitant large vessel GCA and exclude other relevant differentials like infection and malignancy. This atlas provides a contemporary depiction of PMR's pathology and outlines how this knowledge translates into a pattern of findings on whole body 18F-FDG PET/CT that can reliably confirm its diagnosis.
Keywords: diagnosis; imaging; pathology; polymyalgia rheumatica; whole-body positron emission tomography/computed tomography.
© The Author(s) 2024. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures

Similar articles
-
Role of 18F-FDG PET/CT in Large Vessel Vasculitis and Polymyalgia Rheumatica.J Nucl Med. 2023 Apr;64(4):515-521. doi: 10.2967/jnumed.122.265016. J Nucl Med. 2023. PMID: 37011940
-
18F-Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography Findings of Polymyalgia Rheumatica in Patients with Giant Cell Arteritis.J Clin Med. 2023 Nov 8;12(22):6983. doi: 10.3390/jcm12226983. J Clin Med. 2023. PMID: 38002597 Free PMC article.
-
Whole-Body [18F]FDG PET/CT Can Alter Diagnosis in Patients with Suspected Rheumatic Disease.Diagnostics (Basel). 2021 Nov 9;11(11):2073. doi: 10.3390/diagnostics11112073. Diagnostics (Basel). 2021. PMID: 34829421 Free PMC article.
-
Role and potential of 18F-fluorodeoxyglucose-positron emission tomography-computed tomography in large-vessel vasculitis: a comprehensive review.Front Med (Lausanne). 2024 Aug 7;11:1432865. doi: 10.3389/fmed.2024.1432865. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39170047 Free PMC article. Review.
-
Novel PET Imaging of Inflammatory Targets and Cells for the Diagnosis and Monitoring of Giant Cell Arteritis and Polymyalgia Rheumatica.Front Med (Lausanne). 2022 Jun 6;9:902155. doi: 10.3389/fmed.2022.902155. eCollection 2022. Front Med (Lausanne). 2022. PMID: 35733858 Free PMC article. Review.
Cited by
-
Modifiable risk factors and inflammation-related proteins in polymyalgia rheumatica: genome-wide meta-analysis and Mendelian randomisation.Rheumatology (Oxford). 2024 May 24:keae308. doi: 10.1093/rheumatology/keae308. Online ahead of print. Rheumatology (Oxford). 2024. PMID: 38788669 Free PMC article.
-
Norwegian society of rheumatology recommendations on diagnosis and treatment of patients with Polymyalgia Rheumatica: a narrative review.BMC Rheumatol. 2024 Nov 4;8(1):58. doi: 10.1186/s41927-024-00422-6. BMC Rheumatol. 2024. PMID: 39490996 Free PMC article.
-
The DANIsh VASculitis cohort study: protocol for a national multicenter prospective study including incident and prevalent patients with giant cell arteritis and polymyalgia rheumatica.Front Med (Lausanne). 2024 Jul 3;11:1415076. doi: 10.3389/fmed.2024.1415076. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39026552 Free PMC article.
-
Positron Emission Tomography/Computed Tomography in Polymyalgia Rheumatica: When and for What-A Critical Review.Diagnostics (Basel). 2024 Jul 17;14(14):1539. doi: 10.3390/diagnostics14141539. Diagnostics (Basel). 2024. PMID: 39061676 Free PMC article. Review.
-
[News on the imaging of large vessel vasculitis].Z Rheumatol. 2024 Dec;83(10):800-811. doi: 10.1007/s00393-024-01565-0. Epub 2024 Sep 13. Z Rheumatol. 2024. PMID: 39271483 Review. German.
References
-
- Owen CE, Liew DFL, Buchanan RRC.. Musculotendinous inflammation: the defining pathology of polymyalgia rheumatica? J Rheumatol 2019;46:1552–5. - PubMed
-
- Koski JM. Ultrasonographic evidence of synovitis in axial joints in patients with polymyalgia rheumatica. Br J Rheumatol 1992;31:201–3. - PubMed
-
- Meliconi R, Pulsatelli L, Uguccioni M. et al. Leukocyte infiltration in synovial tissue from the shoulder of patients with polymyalgia rheumatica. Quantitative analysis and influence of corticosteroid treatment. Arthritis Rheumatol 1996;39:1199–207. - PubMed
Publication types
LinkOut - more resources
Full Text Sources