

Intentional intoxication with monkshood plant leading to atrioventricular dissociation and ventricular ectopy in a 17-year-old female: a case report
- PMID: 38331724
- PMCID: PMC10851478
- DOI: 10.1186/s12245-024-00588-3
Intentional intoxication with monkshood plant leading to atrioventricular dissociation and ventricular ectopy in a 17-year-old female: a case report
Abstract
Background: Monkshood, a toxic plant containing a potent cardio- and neurotoxin called aconitine, can lead to a range of symptoms, including nausea, vomiting, dizziness, seizures, and cardiac arrhythmias. Mortality associated with this intoxication are due to ventricular tachyarrhythmias which are difficult to treat and often refractory in nature.
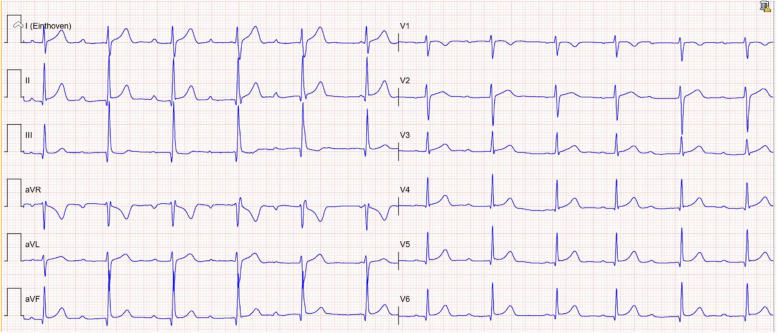
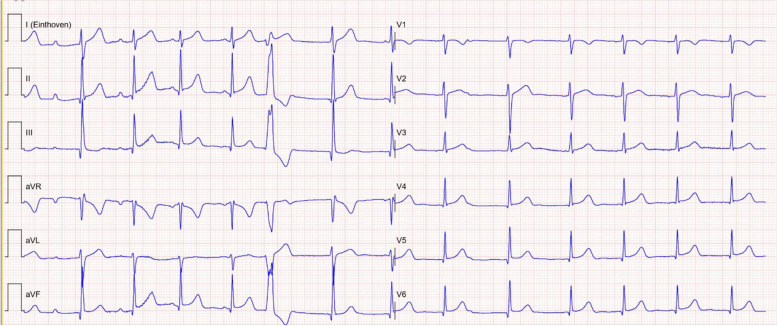
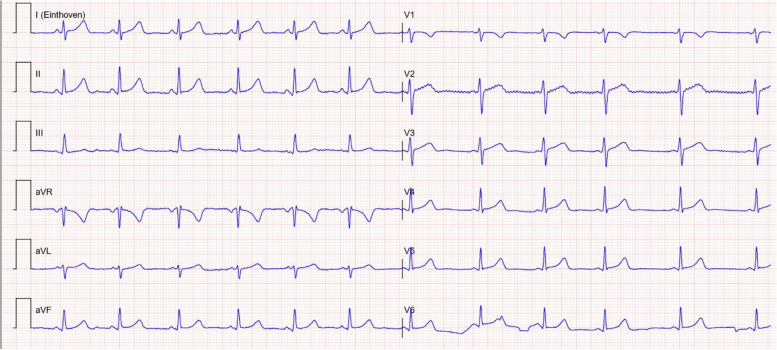
Case presentation: We present a case of a 17-year-old female patient who presented to the emergency department after intentionally ingesting a monkshood plant and developed atrioventricular dissociation and frequent ventricular ectopy. The patient was successfully treated with activated charcoal, supportive care, and cardiac monitoring.
Conclusion: This case highlights the importance of early recognition of aconitine poisoning and the need for prompt supportive care, cardiac rhythm monitoring, and preemptive antiarrhythmic treatment planning.
Keywords: AV dissociation; Aconitine; Arrythmia; Emergency medicine; Monkshood plant; Poisoning.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
[Intoxication with Monkshood (Aconitum napellus)].Ned Tijdschr Geneeskd. 2009;153:A387. Ned Tijdschr Geneeskd. 2009. PMID: 19785799 Dutch.
-
Aconite poisoning.Clin Toxicol (Phila). 2009 Apr;47(4):279-85. doi: 10.1080/15563650902904407. Clin Toxicol (Phila). 2009. PMID: 19514874 Review.
-
[Aconitine poisoning due to confusion of aconite leaves with lovage].Anaesthesist. 2021 Aug;70(8):633-638. doi: 10.1007/s00101-021-01002-w. Epub 2021 Jul 12. Anaesthesist. 2021. PMID: 34251482 German.
-
[Acute Monkshood Intoxication Requiring Acute Resuscitation in Suicidal Intent].Anasthesiol Intensivmed Notfallmed Schmerzther. 2017 Sep;52(9):641-644. doi: 10.1055/s-0043-106283. Epub 2017 Sep 8. Anasthesiol Intensivmed Notfallmed Schmerzther. 2017. PMID: 28886613 German.
-
The management of ventricular dysrhythmia in aconite poisoning.Clin Toxicol (Phila). 2017 Jun;55(5):313-321. doi: 10.1080/15563650.2017.1291944. Epub 2017 Feb 20. Clin Toxicol (Phila). 2017. PMID: 28421842 Review.
References
LinkOut - more resources
Full Text Sources
