

Brentuximab vedotin as a bridge to combination chemotherapy in gray zone lymphoma with severe liver impairment: a case report
- PMID: 38313213
- PMCID: PMC10834647
- DOI: 10.3389/fonc.2023.1254256
Brentuximab vedotin as a bridge to combination chemotherapy in gray zone lymphoma with severe liver impairment: a case report
Abstract
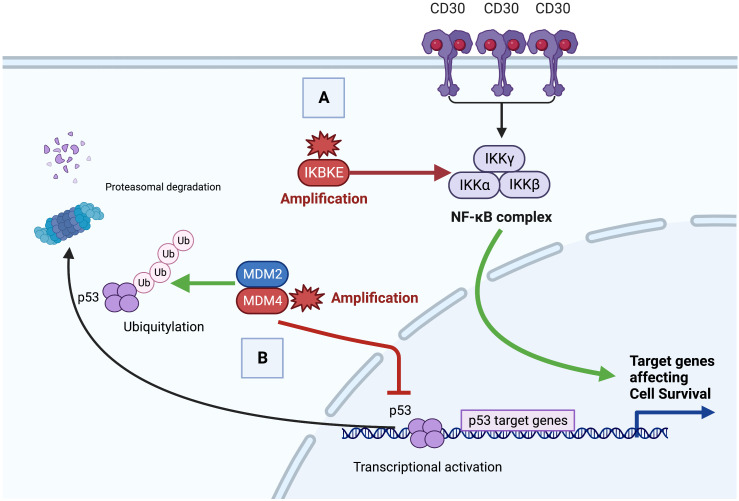
Background: Gray zone lymphoma (GZL) is a rare lymphoma subtype characterized by features intermediate between diffuse large B-cell lymphoma (DLBCL) and classic Hodgkin lymphoma (cHL). The optimal first-line treatment for GZL remains undefined, particularly for patients with poor performance status or baseline organ impairment. Brentuximab vedotin (BV), a targeted therapy that binds to CD30, a TNFR superfamily member involved in NF-kB signaling, has shown promise in the treatment of CD30-positive lymphomas. However, its use in GZL, especially in patients with severe liver impairment, has not been reported previously.
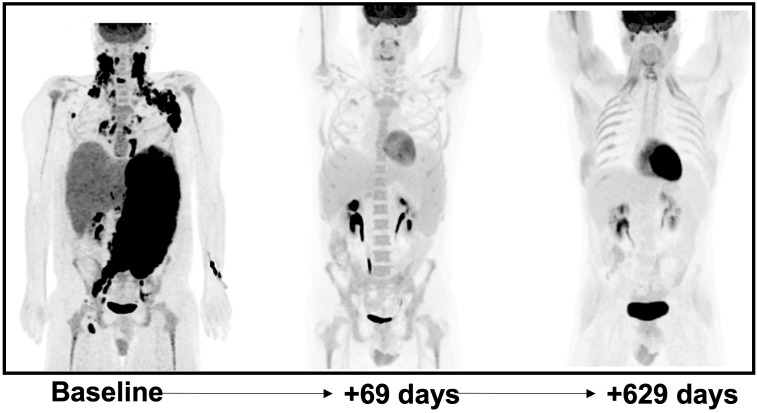
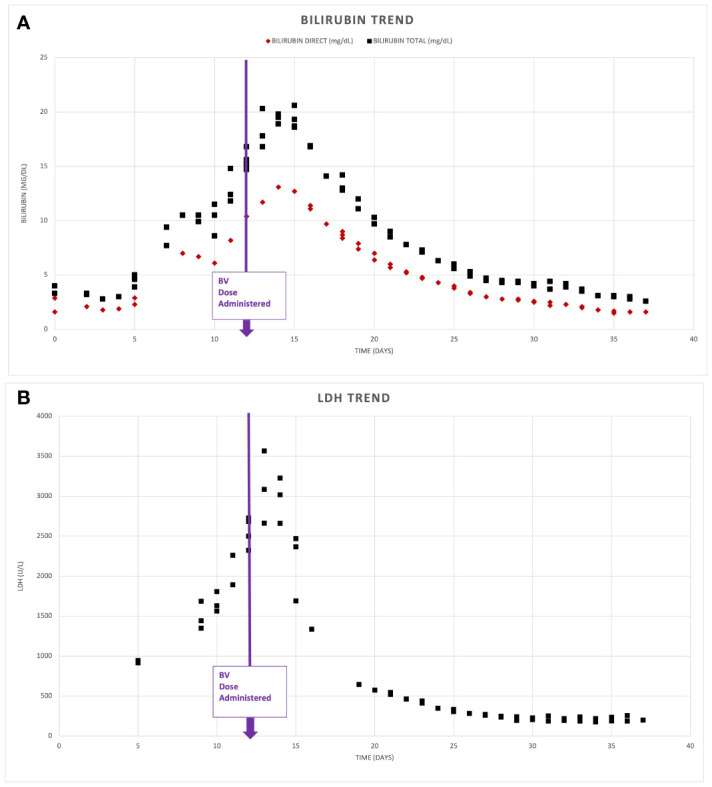
Case description: We present a case of a 37-year-old male with GZL and severe liver impairment at initial presentation. The patient initially received monotherapy with BV, which resulted in a marked improvement in liver enzymes and bilirubin levels. Subsequently, combination cytotoxic chemotherapy consisting of dose-adjusted etoposide, prednisone, cyclophosphamide, and doxorubicin (DA-EP_CH) was added. Repeat imaging revealed near complete resolution of lymphadenopathy and significant reduction in hepatosplenomegaly. The patient completed a full course of chemotherapy and achieved a complete response. Follow-up examinations showed no evidence of recurrent disease, and the patient resumed full-time work.
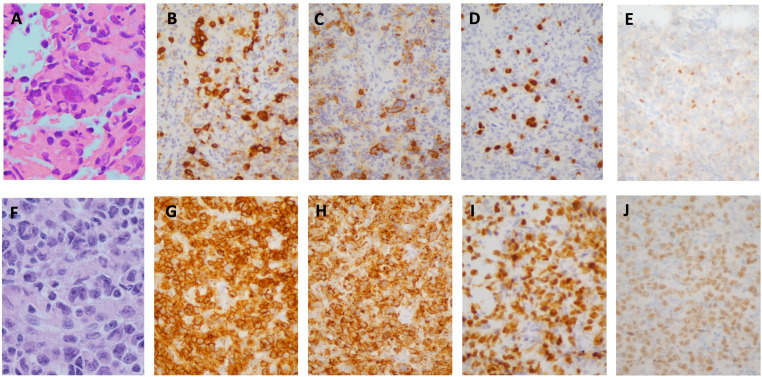
Discussion: GZL poses diagnostic challenges due to its overlapping features with DLBCL and cHL. Accurate diagnosis relies on comprehensive histopathological evaluation, immunophenotyping, and molecular analysis. The optimal first-line treatment for GZL remains uncertain. BV shows promise as an addition to chemotherapy in GZL, even in the presence of severe liver impairment. The molecular pathogenesis of GZL is complex and heterogeneous, frequently involving aberrant NF-kB signaling and impaired apoptosis regulation via loss of TP53 expression. Understanding the underlying molecular mechanisms is essential for developing targeted therapies and identifying predictive biomarkers for treatment response.
Conclusion: This case demonstrates the successful use of BV as a bridge to cytotoxic chemotherapy in a GZL patient with severe liver impairment, highlighting its potential safety and efficacy even in the setting of end-organ failure. Further investigation is warranted to define optimal treatment strategies, identify predictive biomarkers, and improve outcomes for patients with this rare and challenging lymphoma subtype.
Keywords: CD30+ lymphoma; IKBKE; Mdm4; hyperbilirubinemia; targeted therapy.
Copyright © 2024 Asrani, Cengiz, Petersen, Anagnostou and Brody.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
A Rare Case of Grey Zone Lymphoma Successfully Treated with Brentuximab Vedotin and R-CHP Chemotherapy.Case Rep Oncol Med. 2019 Apr 11;2019:4121234. doi: 10.1155/2019/4121234. eCollection 2019. Case Rep Oncol Med. 2019. PMID: 31110830 Free PMC article.
-
Brentuximab vedotin plus AVD followed by involved-node radiotherapy in a patient with classic Hodgkin lymphoma following gray zone lymphoma after autologous stem-cell transplantation failure.Hematology. 2023 Dec;28(1):2207946. doi: 10.1080/16078454.2023.2207946. Hematology. 2023. PMID: 37183912
-
Brentuximab vedotin maintenance after autologous stem cell transplantation for refractory gray zone lymphoma with long-term remission.Mol Clin Oncol. 2021 Jun;14(6):125. doi: 10.3892/mco.2021.2287. Epub 2021 Apr 23. Mol Clin Oncol. 2021. PMID: 33936598 Free PMC article.
-
How I manage patients with grey zone lymphoma.Br J Haematol. 2016 Aug;174(3):345-50. doi: 10.1111/bjh.14174. Epub 2016 Jun 15. Br J Haematol. 2016. PMID: 27301470 Review.
-
Mediastinal large B cell lymphoma and surrounding gray areas: a report of the lymphoma workshop of the 20th meeting of the European Association for Haematopathology.Virchows Arch. 2023 Dec;483(6):733-749. doi: 10.1007/s00428-023-03550-5. Epub 2023 Aug 2. Virchows Arch. 2023. PMID: 37530791 Free PMC article. Review.
References
-
- Qasrawi A, Swofford B, Abughanimeh O, Hildebrandt GC. Trends and outcomes of gray zone lymphoma in the United States: A population-based registry study. Biol Blood Marrow Transplant (2020) 26(3):S230. doi: 10.1016/j.bbmt.2019.12.471 - DOI
-
- Evens AM, Kanakry JA, Sehn LH, Kritharis A, Feldman T, Kroll A, et al. . Gray zone lymphoma with features intermediate between classical Hodgkin lymphoma and diffuse large B-cell lymphoma: characteristics, outcomes, and prognostication among a large multicenter cohort. Am J Hematol (2015) 90(9):778–83. doi: 10.1002/ajh.24082 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous