

Farnesyl-transferase inhibitors show synergistic anticancer effects in combination with novel KRAS-G12C inhibitors
- PMID: 38278976
- PMCID: PMC10951297
- DOI: 10.1038/s41416-024-02586-x
Farnesyl-transferase inhibitors show synergistic anticancer effects in combination with novel KRAS-G12C inhibitors
Abstract
Background: Inhibition of mutant KRAS challenged cancer research for decades. Recently, allele-specific inhibitors were approved for the treatment of KRAS-G12C mutant lung cancer. However, de novo and acquired resistance limit their efficacy and several combinations are in clinical development. Our study shows the potential of combining G12C inhibitors with farnesyl-transferase inhibitors.
Methods: Combinations of clinically approved farnesyl-transferase inhibitors and KRAS G12C inhibitors are tested on human lung, colorectal and pancreatic adenocarcinoma cells in vitro in 2D, 3D and subcutaneous xenograft models of lung adenocarcinoma. Treatment effects on migration, proliferation, apoptosis, farnesylation and RAS signaling were measured by histopathological analyses, videomicroscopy, cell cycle analyses, immunoblot, immunofluorescence and RAS pulldown.
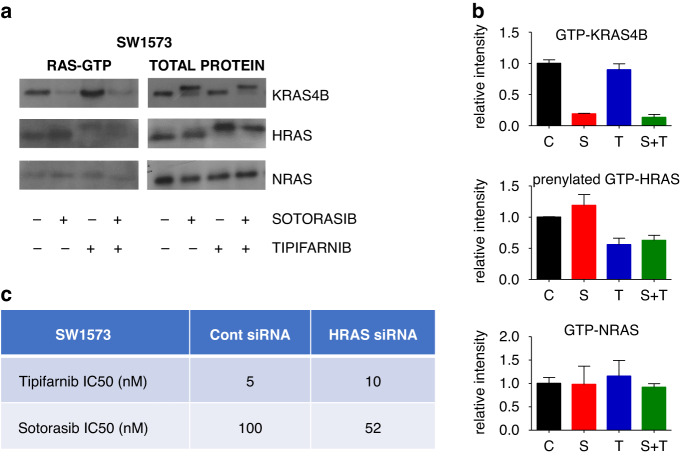
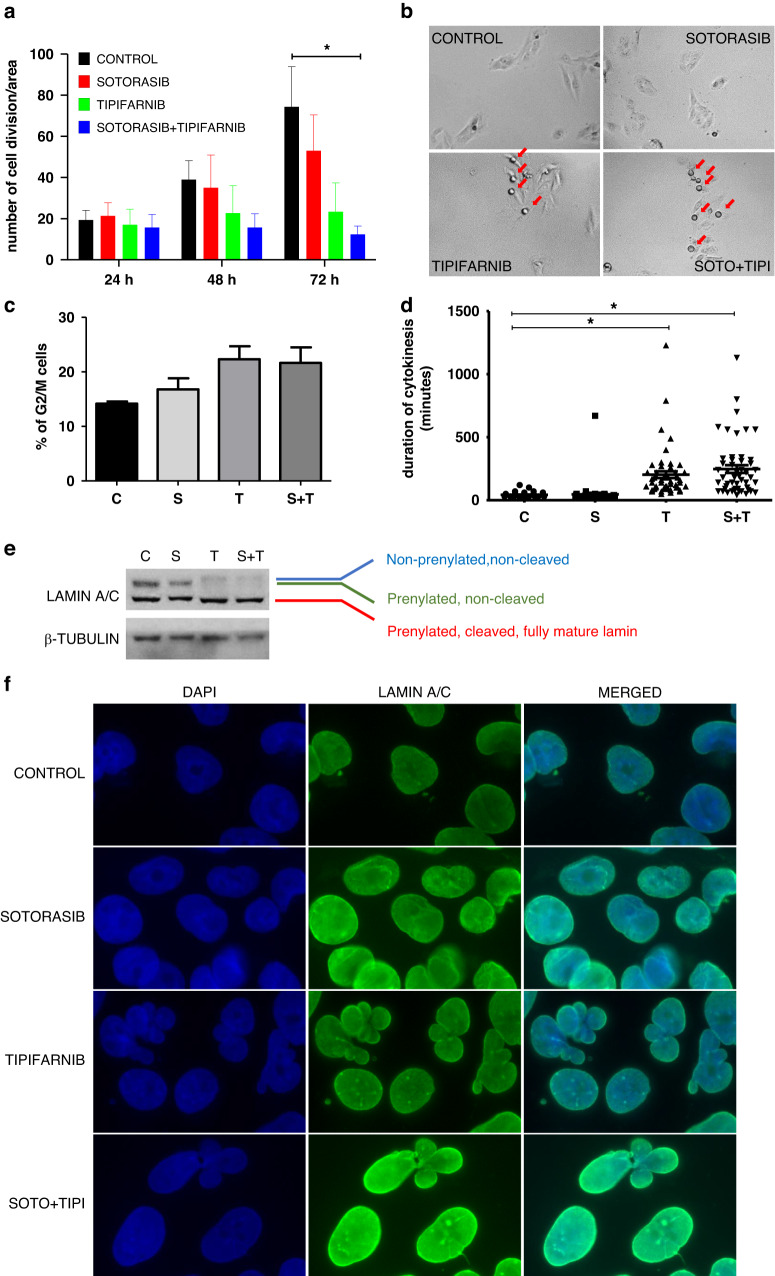
Results: Combination of tipifarnib with sotorasib shows synergistic inhibitory effects on lung adenocarcinoma cells in vitro in 2D and 3D. Mechanistically, we present antiproliferative effect of the combination and interference with compensatory HRAS activation and RHEB and lamin farnesylation. Enhanced efficacy of sotorasib in combination with tipifarnib is recapitulated in the subcutaneous xenograft model of lung adenocarcinoma. Finally, combination of additional KRAS G1C and farnesyl-transferase inhibitors also shows synergism in lung, colorectal and pancreatic adenocarcinoma cellular models.
Discussion: Our findings warrant the clinical exploration of KRAS-G12C inhibitors in combination with farnesyl-transferase inhibitors.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that MB, EM, JTímár, JTóvári, IR and BH filed an international patent for the combinational treatment of
Figures



Similar articles
-
BCL-XL PROTAC degrader DT2216 synergizes with sotorasib in preclinical models of KRASG12C-mutated cancers.J Hematol Oncol. 2022 Mar 9;15(1):23. doi: 10.1186/s13045-022-01241-3. J Hematol Oncol. 2022. PMID: 35260176 Free PMC article.
-
KRAS Inhibitor Resistance in MET-Amplified KRAS G12C Non-Small Cell Lung Cancer Induced By RAS- and Non-RAS-Mediated Cell Signaling Mechanisms.Clin Cancer Res. 2021 Oct 15;27(20):5697-5707. doi: 10.1158/1078-0432.CCR-21-0856. Epub 2021 Aug 7. Clin Cancer Res. 2021. PMID: 34365406
-
Inhibitor of the Nuclear Transport Protein XPO1 Enhances the Anticancer Efficacy of KRAS G12C Inhibitors in Preclinical Models of KRAS G12C-Mutant Cancers.Cancer Res Commun. 2022 May;2(5):342-352. doi: 10.1158/2767-9764.crc-21-0176. Epub 2022 May 10. Cancer Res Commun. 2022. PMID: 35573474 Free PMC article.
-
Sotorasib: a treatment for non-small cell lung cancer with the KRAS G12C mutation.Drugs Today (Barc). 2022 Apr;58(4):175-185. doi: 10.1358/dot.2022.58.4.3400573. Drugs Today (Barc). 2022. PMID: 35412531 Review.
-
KRASG12C mutant lung adenocarcinoma: unique biology, novel therapies and new challenges.Pathol Oncol Res. 2024 Jan 4;29:1611580. doi: 10.3389/pore.2023.1611580. eCollection 2023. Pathol Oncol Res. 2024. PMID: 38239281 Free PMC article. Review.
Cited by
-
Differential effects of hypoxia on motility using various in vitro models of lung adenocarcinoma.Sci Rep. 2024 Sep 3;14(1):20482. doi: 10.1038/s41598-024-70769-w. Sci Rep. 2024. PMID: 39227650 Free PMC article.
References
MeSH terms
Substances
Grants and funding
- ÚNKP-20-3-II/Nemzeti Kutatási, Fejlesztési és Innovációs Hivatal (NKFI Office)
- ÚNKP-21-4-I-SE-24/Nemzeti Kutatási, Fejlesztési és Innovációs Hivatal (NKFI Office)
- ÚNKP-22-4-II-SE-11/Nemzeti Kutatási, Fejlesztési és Innovációs Hivatal (NKFI Office)
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
