

Across-species benefits of adrenalectomy on congenital generalized lipoatrophic diabetes: a review
- PMID: 38260129
- PMCID: PMC10801166
- DOI: 10.3389/fendo.2023.1151873
Across-species benefits of adrenalectomy on congenital generalized lipoatrophic diabetes: a review
Abstract
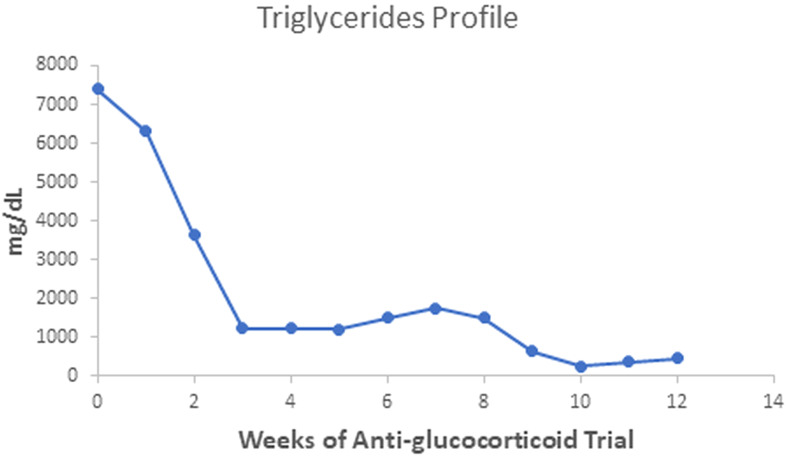
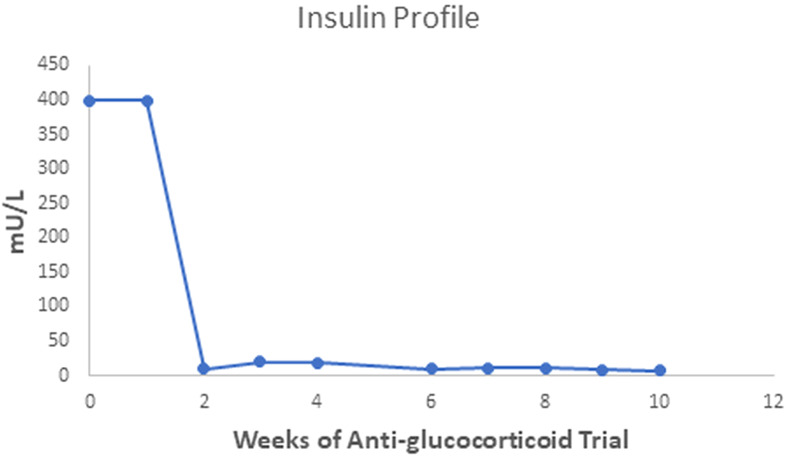
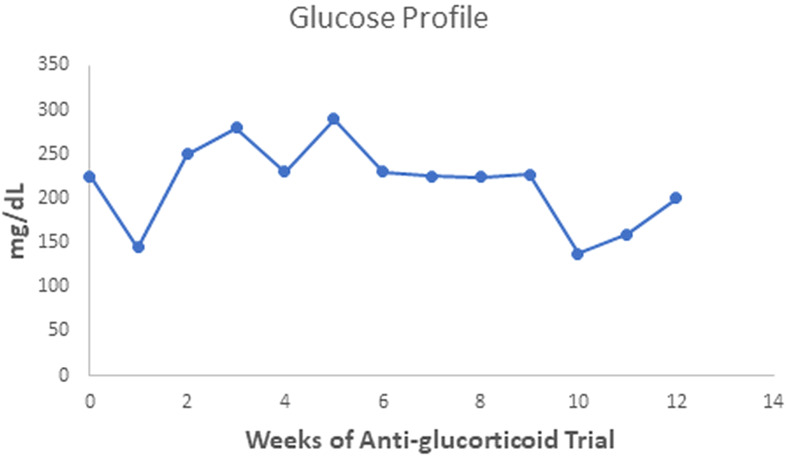
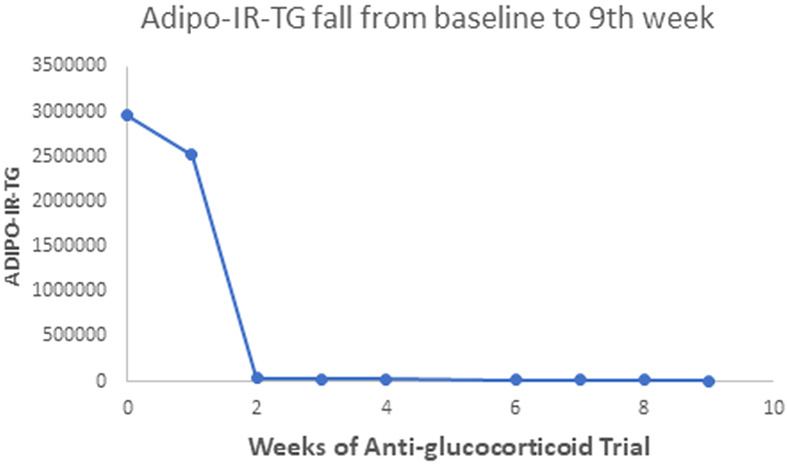
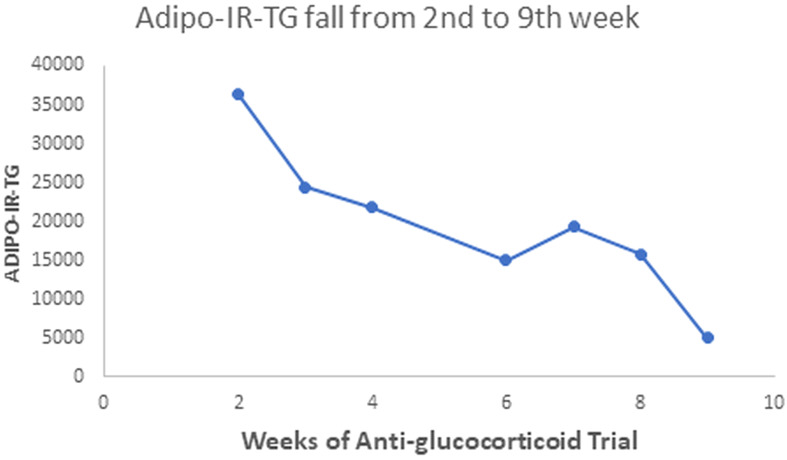
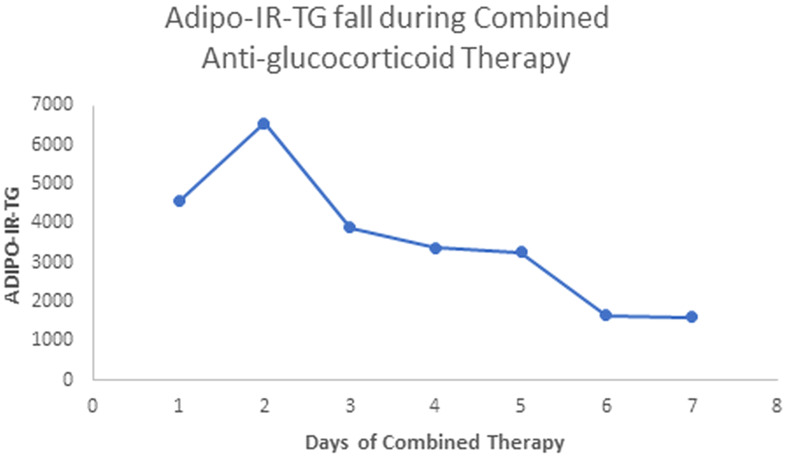
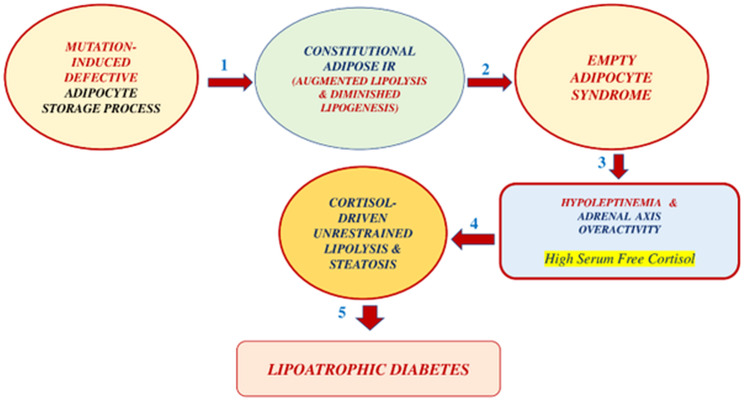
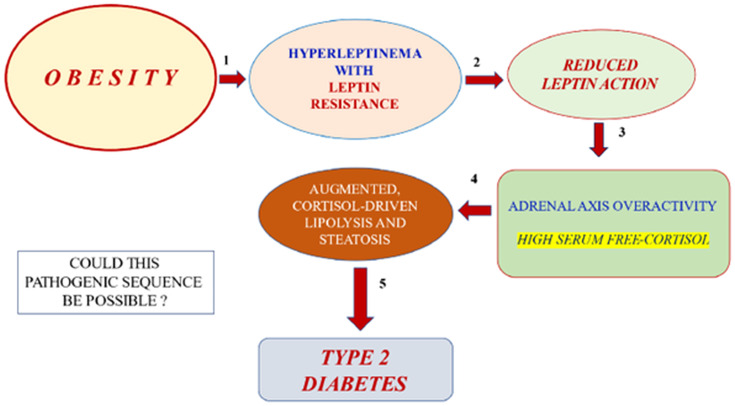
Two adrenalectomies py -45erformed fourteen years apart notoriously alleviated insulin resistance in a female teenager with Congenital Generalized Lipoatrophy (CGL, 1988) and in a murine model of CGL (2002). Following a successful therapeutic trial with anti-glucocorticoids, we performed the first surgical procedure on an 18-year-old girl. Before surgery, the anti-glucocorticoid therapy produced a rapid and striking drop in fasting serum insulin levels (from over 400 to 7.0 mU/L) and a slower -but impressive- fall in fasting serum triglycerides from 7,400 to 220-230 mg/dL. In contrast, fasting serum glucose levels dropped more slowly, from 225-290 to 121-138 mg/dL. Two weeks following total adrenalectomy, the fasting serum glucose level was 98 mg/dL, with a corresponding serum insulin level of 10 mU/L. During an Oral Glucose Tolerance Test, the 2-hour serum glucose was 210 mg/dL, and serum insulin values during the test did not exceed 53 mU/L. In 2002, the A-ZIP/F1 hypoleptinemic mouse had its adrenal glands removed. Even though this CGL model does not respond well to leptin replacement, an infusion of recombinant leptin reduced the characteristic hypercorticosteronemia of this murine model of CGL. Adrenalectomy in this transgenic mouse improved insulin sensitivity in the liver and muscle. In summary, adrenalectomy -in both a human and a mouse case of CGL- limited adipose tissue exposure to corticosteroid action and led to a notorious metabolic improvement. On a broader scenario, given that leptin restrains the adrenal axis, the reduced leptin activity of the leptin resistance displayed by obese subjects should lead to adrenal axis overactivity. This overactivity should result in elevated serum levels of free cortisol, free fatty acids, and glycerol. In this manner, leptin resistance should lead to peripheral (adipose tissue, liver, and muscle) insulin resistance and islet beta-cell apoptosis, paving the way to Type 2 diabetes.
Keywords: Berardinelli-Seip syndrome; Ketoconazole; RU-486; adipose insulin resistance; adrenalectomy; anti-glucocorticoid therapy.
Copyright © 2024 Contreras and Vigil.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Adrenalectomy improves diabetes in A-ZIP/F-1 lipoatrophic mice by increasing both liver and muscle insulin sensitivity.Diabetes. 2002 Jul;51(7):2113-8. doi: 10.2337/diabetes.51.7.2113. Diabetes. 2002. PMID: 12086940
-
Metabolic correction induced by leptin replacement treatment in young children with Berardinelli-Seip congenital lipoatrophy.Pediatrics. 2007 Aug;120(2):e291-6. doi: 10.1542/peds.2006-3165. Pediatrics. 2007. PMID: 17671040 Clinical Trial.
-
Transgenic overexpression of leptin rescues insulin resistance and diabetes in a mouse model of lipoatrophic diabetes.Diabetes. 2001 Jun;50(6):1440-8. doi: 10.2337/diabetes.50.6.1440. Diabetes. 2001. PMID: 11375346
-
[Therapy resistant diabetes mellitus and lipodystrophy: leptin therapy leads to improvement].Ned Tijdschr Geneeskd. 2013;157(4):A5482. Ned Tijdschr Geneeskd. 2013. PMID: 23343738 Review. Dutch.
-
Lipoatrophic diabetes: a case report with a brief review of the literature.J Adolesc Health. 2009 Jan;44(1):94-5. doi: 10.1016/j.jadohealth.2008.06.007. Epub 2008 Sep 27. J Adolesc Health. 2009. PMID: 19101466 Review.
References
-
- Mantzoros CS. Lipodystrophic syndromes. Uptodate (2023).
-
- Contreras PH. Berardinelli-Seip Syndrome: Report of an Old Case Successfully Treated with Anti-Glucocorticoid Therapy Followed by Bilateral Adrenalectomy. Chapter 7. In: Infante M, editor. Evolving Concepts in Insulin Resistance. (London, UK: Intechopen; ) (2022). p. 159–78.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials