

Alterations in Th17 Cells and Non-Classical Monocytes as a Signature of Subclinical Coronary Artery Atherosclerosis during ART-Treated HIV-1 Infection
- PMID: 38247848
- PMCID: PMC10813976
- DOI: 10.3390/cells13020157
Alterations in Th17 Cells and Non-Classical Monocytes as a Signature of Subclinical Coronary Artery Atherosclerosis during ART-Treated HIV-1 Infection
Abstract
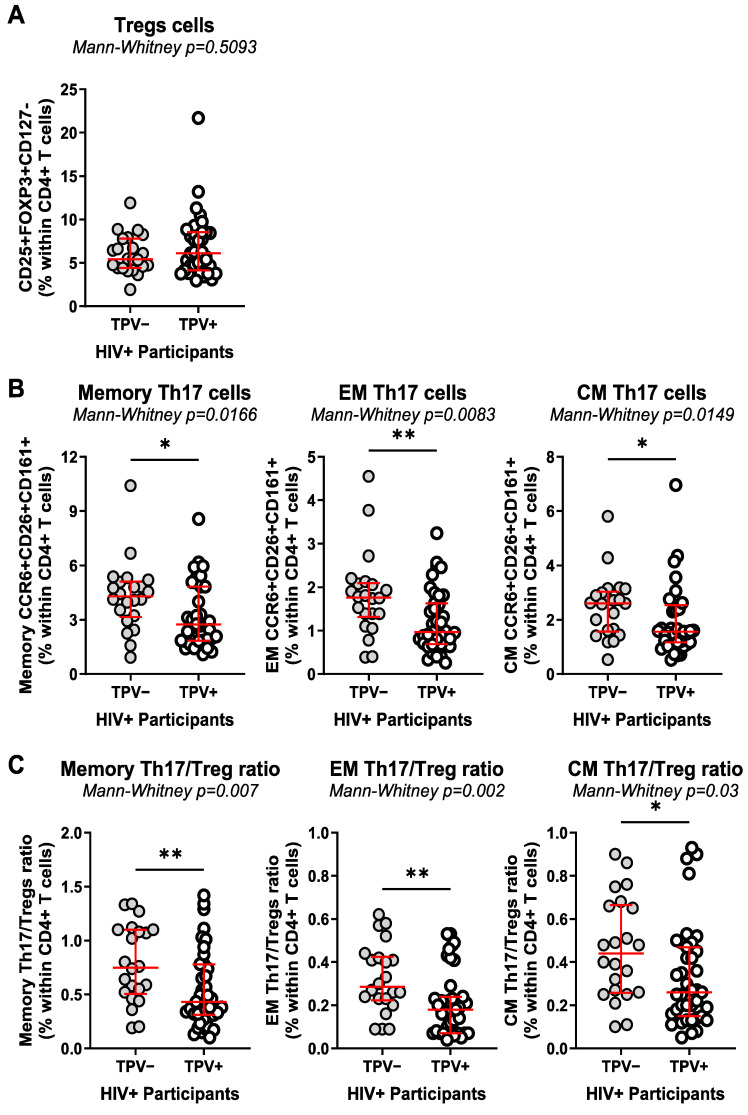
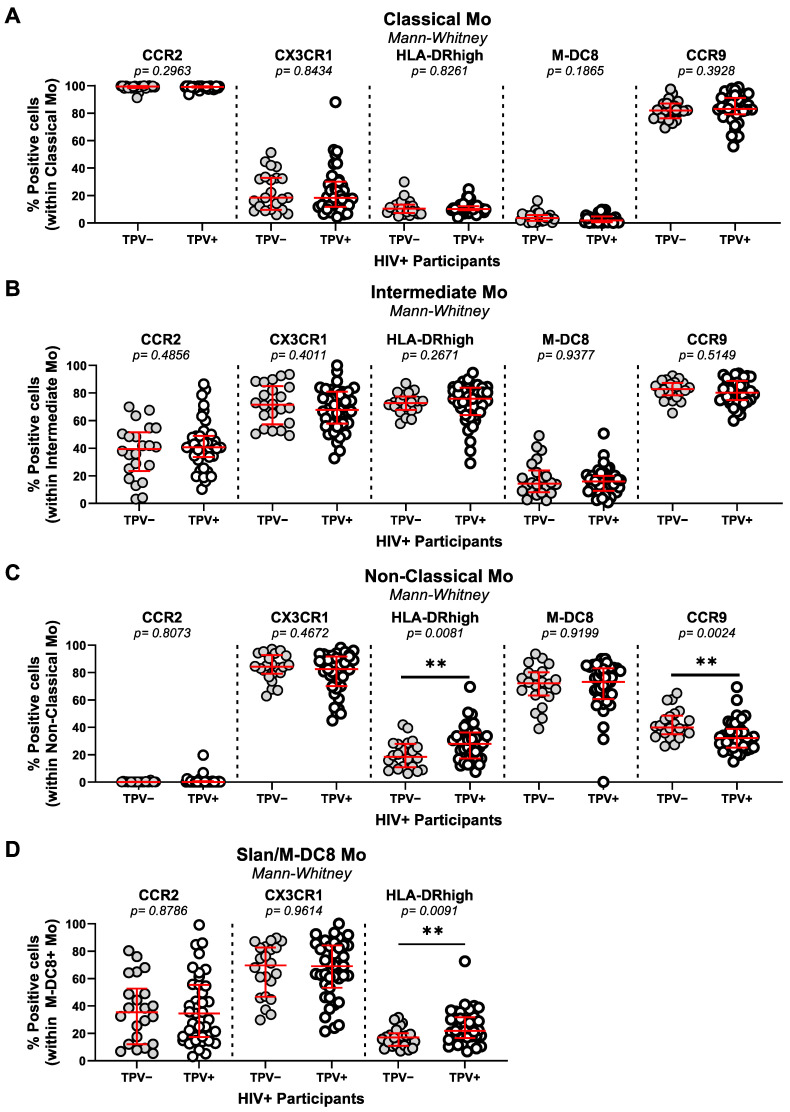
Cardiovascular disease (CVD) remains an important comorbidity in people living with HIV-1 (PLWH) receiving antiretroviral therapy (ART). Our previous studies performed in the Canadian HIV/Aging Cohort Study (CHACS) (>40 years-old; Framingham Risk Score (FRS) > 5%) revealed a 2-3-fold increase in non-calcified coronary artery atherosclerosis (CAA) plaque burden, measured by computed tomography angiography scan (CTAScan) as the total (TPV) and low attenuated plaque volume (LAPV), in ART-treated PLWH (HIV+) versus uninfected controls (HIV-). In an effort to identify novel correlates of subclinical CAA, markers of intestinal damage (sCD14, LBP, FABP2); cell trafficking/inflammation (CCL20, CX3CL1, MIF, CCL25); subsets of Th17-polarized and regulatory (Tregs) CD4+ T-cells, classical/intermediate/non-classical monocytes, and myeloid/plasmacytoid dendritic cells were studied in relationship with HIV and TPV/LAPV status. The TPV detection/values coincided with higher plasma sCD14, FABP2, CCL20, MIF, CX3CL1, and triglyceride levels; lower Th17/Treg ratios; and classical monocyte expansion. Among HIV+, TPV+ versus TPV- exhibited lower Th17 frequencies, reduced Th17/Treg ratios, higher frequencies of non-classical CCR9lowHLADRhigh monocytes, and increased plasma fibrinogen levels. Finally, Th17/Treg ratios and non-classical CCR9lowHLADRhigh monocyte frequencies remained associated with TPV/LAPV after adjusting for FRS and HIV/ART duration in a logistic regression model. These findings point to Th17 paucity and non-classical monocyte abundance as novel immunological correlates of subclinical CAA that may fuel the CVD risk in ART-treated PLWH.
Keywords: HIV-1; Th17/Treg cells; antiretroviral therapy (ART); cardiovascular disease (CVD); myeloid/plasmacytoid dendritic cells; non-classical monocytes.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
Similar articles
-
A Blood Immunological Signature of Subclinical Coronary Artery Atherosclerosis in People Living with HIV-1 Receiving Antiretroviral Therapy.bioRxiv [Preprint]. 2023 Dec 18:2023.12.15.571922. doi: 10.1101/2023.12.15.571922. bioRxiv. 2023. PMID: 38187644 Free PMC article. Preprint.
-
Non-Classical Monocytes and Monocyte Chemoattractant Protein-1 (MCP-1) Correlate with Coronary Artery Calcium Progression in Chronically HIV-1 Infected Adults on Stable Antiretroviral Therapy.PLoS One. 2016 Feb 11;11(2):e0149143. doi: 10.1371/journal.pone.0149143. eCollection 2016. PLoS One. 2016. PMID: 26867220 Free PMC article.
-
Elevated levels of monocyte activation markers are associated with subclinical atherosclerosis in men with and those without HIV infection.J Infect Dis. 2015 Apr 15;211(8):1219-28. doi: 10.1093/infdis/jiu594. Epub 2014 Oct 30. J Infect Dis. 2015. PMID: 25362192 Free PMC article.
-
How Monocytes Contribute to Increased Risk of Atherosclerosis in Virologically-Suppressed HIV-Positive Individuals Receiving Combination Antiretroviral Therapy.Front Immunol. 2019 Jun 19;10:1378. doi: 10.3389/fimmu.2019.01378. eCollection 2019. Front Immunol. 2019. PMID: 31275317 Free PMC article. Review.
-
Th17 CD4+ T-Cell as a Preferential Target for HIV Reservoirs.Front Immunol. 2022 Feb 7;13:822576. doi: 10.3389/fimmu.2022.822576. eCollection 2022. Front Immunol. 2022. PMID: 35197986 Free PMC article. Review.
Cited by
-
Inflammatory and Immune Mechanisms for Atherosclerotic Cardiovascular Disease in HIV.Int J Mol Sci. 2024 Jul 1;25(13):7266. doi: 10.3390/ijms25137266. Int J Mol Sci. 2024. PMID: 39000373 Free PMC article. Review.
References
-
- Boldeanu I., Sadouni M., Mansour S., Baril J.G., Trottier B., Soulez G., Chin S.A., Leipsic J., Tremblay C., Durand M., et al. Prevalence and Characterization of Subclinical Coronary Atherosclerotic Plaque with CT among Individuals with HIV: Results from the Canadian HIV and Aging Cohort Study. Radiology. 2021;299:571–580. doi: 10.1148/radiol.2021203297. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
