

Hemorheological, cardiorespiratory, and cerebrovascular effects of pentoxifylline following acclimatization to 3,800 m
- PMID: 38241007
- PMCID: PMC11221811
- DOI: 10.1152/ajpheart.00783.2023
Hemorheological, cardiorespiratory, and cerebrovascular effects of pentoxifylline following acclimatization to 3,800 m
Abstract
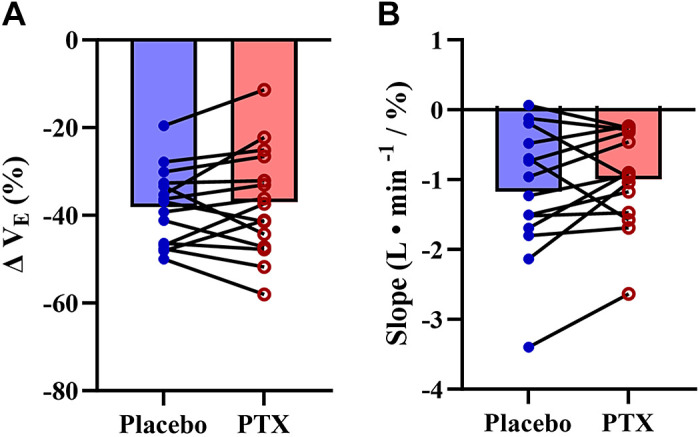
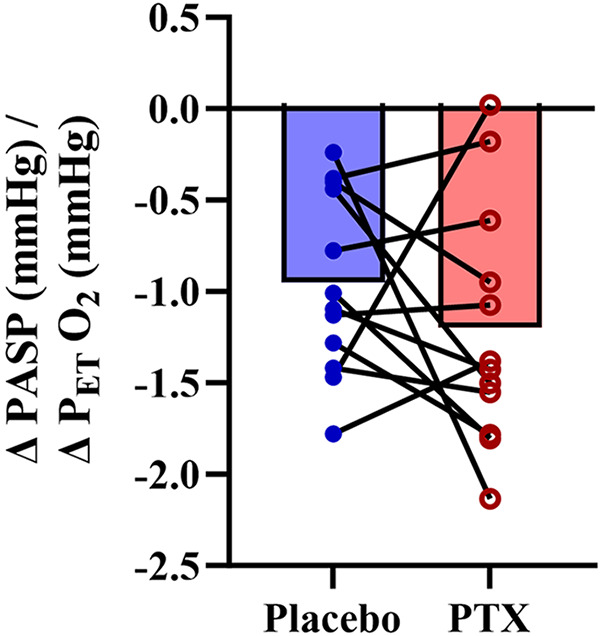
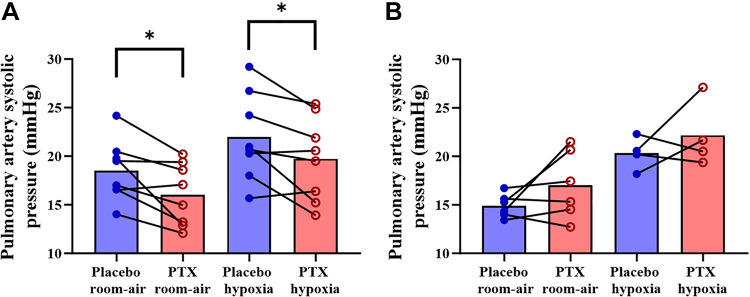
Pentoxifylline is a nonselective phosphodiesterase inhibitor used for the treatment of peripheral artery disease. Pentoxifylline acts through cyclic adenosine monophosphate, thereby enhancing red blood cell deformability, causing vasodilation and decreasing inflammation, and potentially stimulating ventilation. We conducted a double-blind, placebo-controlled, crossover, counter-balanced study to test the hypothesis that pentoxifylline could lower blood viscosity, enhance cerebral blood flow, and decrease pulmonary artery pressure in lowlanders following 11-14 days at 3,800 m. Participants (6 males/10 females; age, 27 ± 4 yr old) received either a placebo or 400 mg of pentoxifylline orally the night before and again 2 h before testing. We assessed arterial blood gases, venous hemorheology (blood viscosity, red blood cell deformability, and aggregation), and inflammation (TNF-α) in room air (end-tidal oxygen partial pressure, ∼52 mmHg). Global cerebral blood flow (gCBF), ventilation, and pulmonary artery systolic pressure (PASP) were measured in room air and again after 8-10 min of isocapnic hypoxia (end-tidal oxygen partial pressure, 40 mmHg). Pentoxifylline did not alter arterial blood gases, TNF-α, or hemorheology compared with placebo. Pentoxifylline did not affect gCBF or ventilation during room air or isocapnic hypoxia compared with placebo. However, in females, PASP was reduced with pentoxifylline during room air (placebo, 19 ± 3; pentoxifylline, 16 ± 3 mmHg; P = 0.021) and isocapnic hypoxia (placebo, 22 ± 5; pentoxifylline, 20 ± 4 mmHg; P = 0.029), but not in males. Acute pentoxifylline administration in lowlanders at 3,800 m had no impact on arterial blood gases, hemorheology, inflammation, gCBF, or ventilation. Unexpectedly, however, pentoxifylline reduced PASP in female participants, indicating a potential effect of sex on the pulmonary vascular responses to pentoxifylline.NEW & NOTEWORTHY We conducted a double-blind, placebo-controlled study on the rheological, cardiorespiratory and cerebrovascular effects of acute pentoxifylline in healthy lowlanders after 11-14 days at 3,800 m. Although red blood cell deformability was reduced and blood viscosity increased compared with low altitude, acute pentoxifylline administration had no impact on arterial blood gases, hemorheology, inflammation, cerebral blood flow, or ventilation. Pentoxifylline decreased pulmonary artery systolic pressure in female, but not male, participants.
Keywords: cerebral blood flow; chemoreflex; high altitude; hypoxic pulmonary vasoconstriction; red blood cell.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures


Similar articles
-
The influence of hemoconcentration on hypoxic pulmonary vasoconstriction in acute, prolonged, and lifelong hypoxemia.Am J Physiol Heart Circ Physiol. 2021 Oct 1;321(4):H738-H747. doi: 10.1152/ajpheart.00357.2021. Epub 2021 Aug 27. Am J Physiol Heart Circ Physiol. 2021. PMID: 34448634
-
Cardiopulmonary and cerebrovascular acclimatization in children and adults at 3800 m.J Physiol. 2022 Nov;600(22):4849-4863. doi: 10.1113/JP283419. Epub 2022 Oct 17. J Physiol. 2022. PMID: 36165275
-
Adenosine receptor-dependent signaling is not obligatory for normobaric and hypobaric hypoxia-induced cerebral vasodilation in humans.J Appl Physiol (1985). 2017 Apr 1;122(4):795-808. doi: 10.1152/japplphysiol.00840.2016. Epub 2017 Jan 12. J Appl Physiol (1985). 2017. PMID: 28082335 Free PMC article.
-
Pentoxifylline. A review of its pharmacodynamic and pharmacokinetic properties, and its therapeutic efficacy.Drugs. 1987 Jul;34(1):50-97. doi: 10.2165/00003495-198734010-00003. Drugs. 1987. PMID: 3308412 Review.
-
Hypoxia and hemorheological properties in older individuals.Ageing Res Rev. 2022 Aug;79:101650. doi: 10.1016/j.arr.2022.101650. Epub 2022 May 18. Ageing Res Rev. 2022. PMID: 35597435 Review.
References
-
- Tymko MM, Willie CK, Howe CA, Hoiland RL, Stone RM, Tymko K, Tymko C, MacLeod D, Anholm JD, Gasho C, Villafuerte F, Vizcardo-Galindo G, Figueroa-Mujica R, Day TA, Bird JD, Foster GE, Steinback CD, Brugniaux JV, Champigneulle B, Stauffer E, Doutreleau S, Verges S, Swenson ER, Ainslie PN. Acid-base balance at high altitude in lowlanders and indigenous highlanders. J Appl Physiol (1985) 132: 575–580, 2022. doi:10.1152/japplphysiol.00757.2021. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources