

Evaluation of Dermatological and Neurological Aspects of the Relationship between Rosacea and Headaches
- PMID: 38201332
- PMCID: PMC10795644
- DOI: 10.3390/diagnostics14010023
Evaluation of Dermatological and Neurological Aspects of the Relationship between Rosacea and Headaches
Abstract
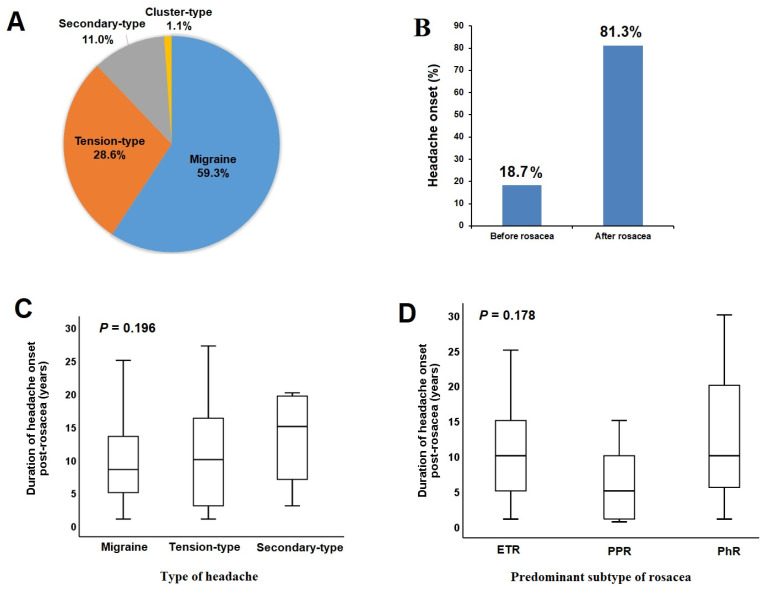
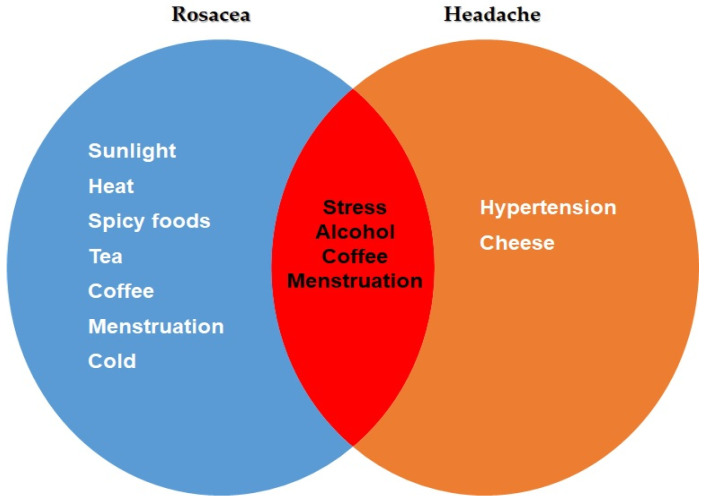
This study aimed to investigate the relationship between rosacea and headaches, focusing on different subtypes, as well as the associated clinical features and triggering factors. In this prospective study, 300 patients diagnosed with rosacea and 320 control subjects without rosacea or any connected mast cell activation illness were included. Patients with rosacea were assessed by a dermatologist according to the 2019 updated rosacea classification (ROSCO panel). Accordingly, patients were classified based on their predominant rosacea subtype as follows: erythematotelangiectatic (ETR), papulopustular (PPR), or phymatous (RhR). Patients experiencing headaches were assessed using the International Headache Classification. Headaches were categorized as migraine, tension-type headaches (TTHs), secondary types (STHs), and cluster-type headaches (CTHs). The ratio of headache was 30.3% in the rosacea group, which did not show a significant difference compared to the control group (30.3% vs. 25.0%, p = 0.138). In 81.3% of rosacea patients with headaches, headache onset occurred after the diagnosis of rosacea. The rate of patients with headaches was higher in the ETR group compared to the PPR and RhR groups (35.2% vs. 16.2% vs. 23.1%, p = 0.007, respectively). In terms of headache subtypes, the rates of patients with migraine and STHs were higher in the ETR group compared to the PPR and RhR groups, while the rate of patients with TTHs was higher in the RhR group. A positive correlation was found between rosacea severity and migraine severity (r = 0.284, p < 0.05). Among the triggering factors for rosacea, only sunlight was found to be associated with headaches. Lower age, female gender, and moderate to severe rosacea severity were identified as independent factors increasing the likelihood of headaches. A significant portion of rosacea patients experience headaches. Particularly, different subtypes of rosacea may be associated with various types of headaches. This study, highlighting the connection between migraine and ETR, is a pioneering work that demonstrates common pathogenic mechanisms and potential triggers.
Keywords: migraine; neurogenic inflammation; primary headaches; rosacea; vascular dysregulation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
An observational cross-sectional survey of rosacea: clinical associations and progression between subtypes.Br J Dermatol. 2013 Sep;169(3):555-62. doi: 10.1111/bjd.12385. Br J Dermatol. 2013. PMID: 23600367
-
Clinicopathological Survey of 204 Rosacea Patients Regarding Rosacea Subgroups and Severity.Dermatol Pract Concept. 2023 Jul 1;13(3):e2023182. doi: 10.5826/dpc.1303a182. Dermatol Pract Concept. 2023. PMID: 37557115 Free PMC article.
-
Exploring the efficacy of laser speckle contrast imaging in the stratified diagnosis of rosacea: a quantitative analysis of facial blood flow dynamics across varied regions.Front Immunol. 2024 Aug 23;15:1419005. doi: 10.3389/fimmu.2024.1419005. eCollection 2024. Front Immunol. 2024. PMID: 39247187 Free PMC article.
-
New insights into rosacea pathophysiology: a review of recent findings.J Am Acad Dermatol. 2013 Dec;69(6 Suppl 1):S15-26. doi: 10.1016/j.jaad.2013.04.045. J Am Acad Dermatol. 2013. PMID: 24229632 Review.
-
Updating the diagnosis, classification and assessment of rosacea: recommendations from the global ROSacea COnsensus (ROSCO) panel.Br J Dermatol. 2017 Feb;176(2):431-438. doi: 10.1111/bjd.15122. Epub 2017 Jan 23. Br J Dermatol. 2017. PMID: 27718519
References
Grants and funding
LinkOut - more resources
Full Text Sources
