

Shear Wave Elastography for Assessing Liver Stiffness in HCV-Infected Kidney Transplant Recipients after Direct-Acting Antiviral Treatment: A Comparative Study with Magnetic Resonance Elastography
- PMID: 38137615
- PMCID: PMC10743898
- DOI: 10.3390/jcm12247547
Shear Wave Elastography for Assessing Liver Stiffness in HCV-Infected Kidney Transplant Recipients after Direct-Acting Antiviral Treatment: A Comparative Study with Magnetic Resonance Elastography
Abstract
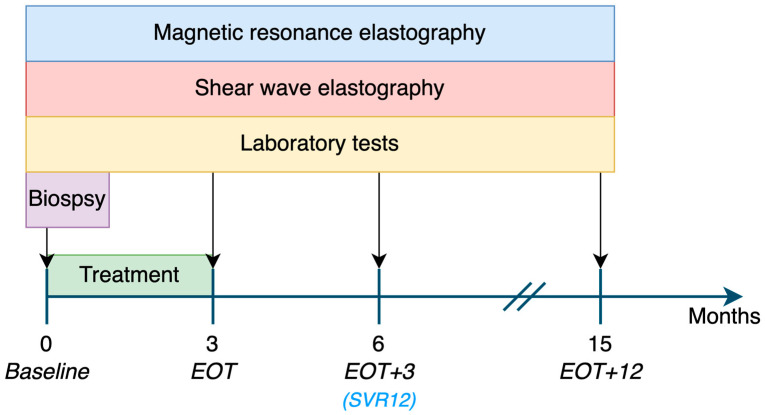
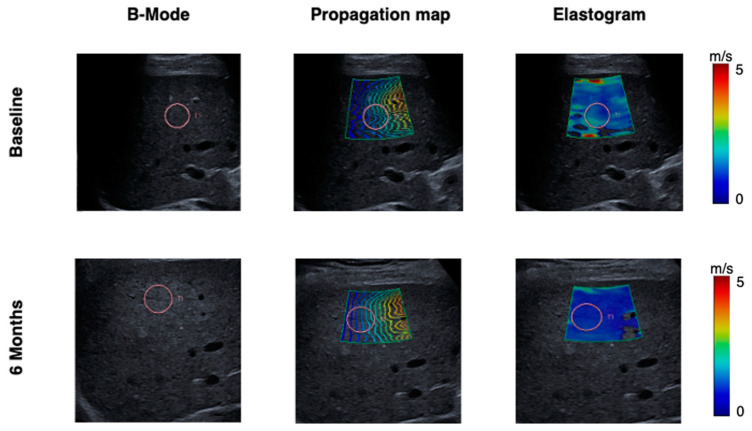
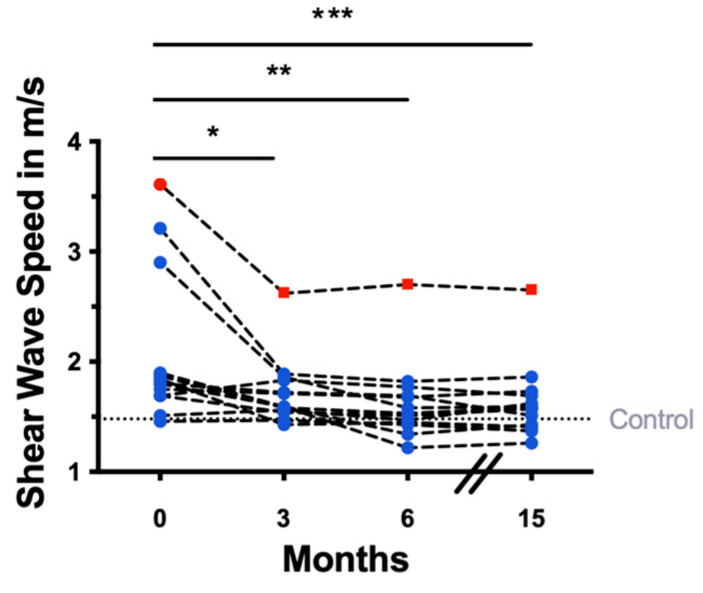
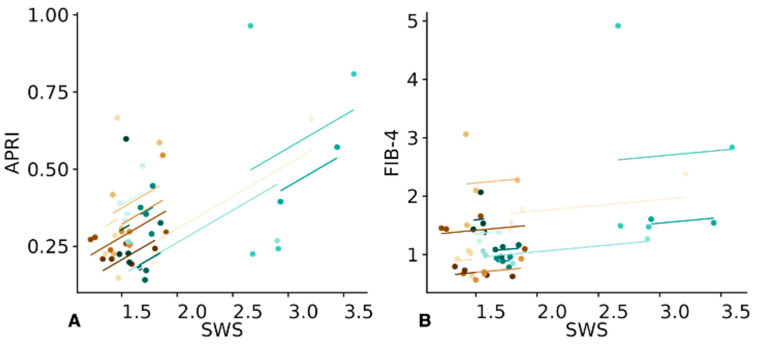
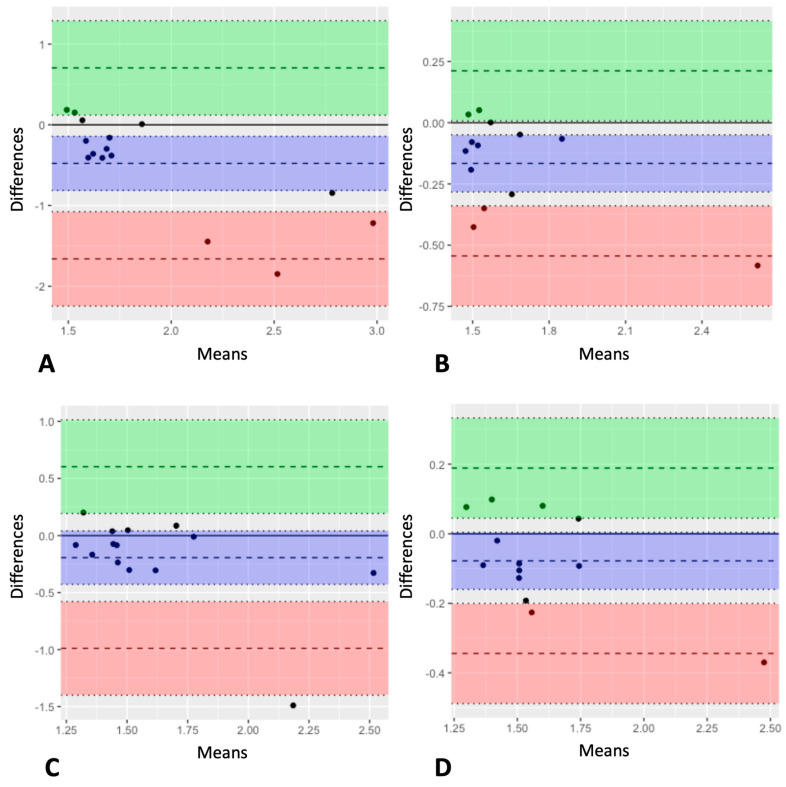
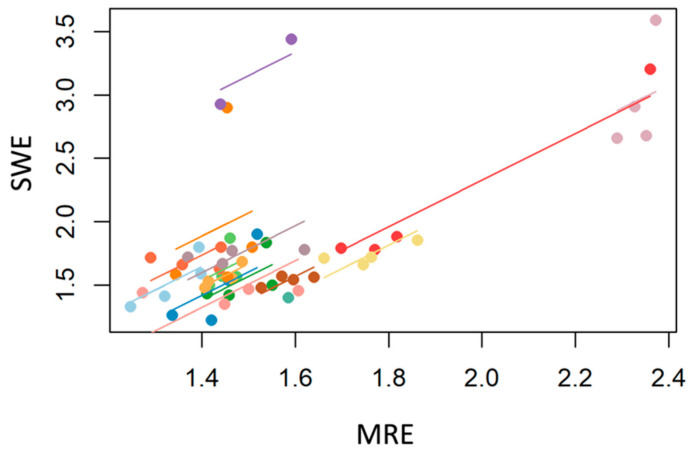
Hepatitis C virus (HCV) infection can lead to hepatic fibrosis. The advent of direct-acting antivirals (DAAs) has substantially improved sustained virological response (SVR) rates. In this context, kidney transplant recipients (KTRs) are of particular interest due to their higher HCV infection rates and uncertain renal excretion and bioavailability of DAAs. We investigated liver stiffness after DAA treatment in 15 HCV-infected KTRs using ultrasound shear wave elastography (SWE) in comparison with magnetic resonance elastography (MRE). KTRs were treated with DAAs (daclatasvir and sofosbuvir) for three months and underwent SWE at baseline, end of therapy (EOT), and 3 (EOT+3) and 12 months (EOT+12) after EOT. Fourteen patients achieved SVR12. Shear wave speed (SWS)-as a surrogate parameter for tissue stiffness-was substantially lower at all three post-therapeutic timepoints compared with baseline (EOT: -0.42 m/s, p < 0.01; CI = -0.75--0.09, EOT+3: -0.43 m/s, p < 0.01; CI = -0.75--0.11, and EOT+12: -0.52 m/s, p < 0.001; CI = -0.84--0.19), suggesting liver regeneration after viral eradication and end of inflammation. Baseline SWS correlated positively with histopathological fibrosis scores (r = 0.48; CI = -0.11-0.85). Longitudinal results correlated moderately with APRI (r = 0.41; CI = 0.12-0.64) but not with FIB-4 scores (r = 0.12; CI = -0.19-0.41). Although higher on average, SWE-derived measurements correlated strongly with MRE (r = 0.64). In conclusion, SWE is suitable for non-invasive therapy monitoring in KTRs with HCV infection.
Keywords: direct-acting antivirals; elastography; hepatitis C; kidney transplant recipients; liver stiffness; magnetic resonance elastography; shear wave elastography; ultrasound elastography.
Conflict of interest statement
I.S. is a patent holder for a technical development related to MR elastography. K.B. reports on the receipt of grants from Bristol Myers Squibb during the study, and T.F. acknowledges receiving honoraria from Canon Medical. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. S.A., F.H., M.D., U.G., E.S., C.E.A., B.H. and S.R.M.G. declare no conflict of interest.
Figures
Similar articles
-
Tomoelastography for Longitudinal Monitoring of Viscoelasticity Changes in the Liver and in Renal Allografts after Direct-Acting Antiviral Treatment in 15 Kidney Transplant Recipients with Chronic HCV Infection.J Clin Med. 2021 Feb 1;10(3):510. doi: 10.3390/jcm10030510. J Clin Med. 2021. PMID: 33535495 Free PMC article.
-
Early fibrosis regression by shear wave elastography after successful direct-acting anti-HCV therapy.Clin Exp Med. 2020 Feb;20(1):143-148. doi: 10.1007/s10238-019-00597-0. Epub 2019 Dec 2. Clin Exp Med. 2020. PMID: 31792631
-
Improvement of liver stiffness in patients with hepatitis C virus infection who received direct-acting antiviral therapy and achieved sustained virological response.J Gastroenterol Hepatol. 2017 Dec;32(12):1982-1988. doi: 10.1111/jgh.13788. J Gastroenterol Hepatol. 2017. PMID: 28299813
-
Significant decrease in liver stiffness detected by two dimensional shear-wave elastography after treatment with direct-acting antiviral agents in patients with chronic Hepatitis C.Turk J Gastroenterol. 2020 Feb;31(2):142-147. doi: 10.5152/tjg.2020.19418. Turk J Gastroenterol. 2020. PMID: 32141823 Free PMC article.
-
Liver Stiffness Evaluation in Chronic Hepatitis C Patients with Cirrhosis before and after Direct-Acting Antivirals.Microorganisms. 2024 Jul 12;12(7):1418. doi: 10.3390/microorganisms12071418. Microorganisms. 2024. PMID: 39065186 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
