

COVID-19 illness severity and 2-year prevalence of physical symptoms: an observational study in Iceland, Sweden, Norway and Denmark
- PMID: 38115966
- PMCID: PMC10730314
- DOI: 10.1016/j.lanepe.2023.100756
COVID-19 illness severity and 2-year prevalence of physical symptoms: an observational study in Iceland, Sweden, Norway and Denmark
Abstract
Background: Although the persistence of physical symptoms after SARS-CoV-2 infection is a major public health concern, evidence from large observational studies beyond one year post diagnosis remain scarce. We aimed to assess the prevalence of physical symptoms in relation to acute illness severity up to more than 2-years after diagnosis of COVID-19.
Methods: This multinational study included 64,880 adult participants from Iceland, Sweden, Denmark, and Norway with self-reported data on COVID-19 and physical symptoms from April 2020 to August 2022. We compared the prevalence of 15 physical symptoms, measured by the Patient Health Questionnaire (PHQ-15), among individuals with or without a confirmed COVID-19 diagnosis, by acute illness severity, and by time since diagnosis. We additionally assessed the change in symptoms in a subset of Swedish adults with repeated measures, before and after COVID-19 diagnosis.
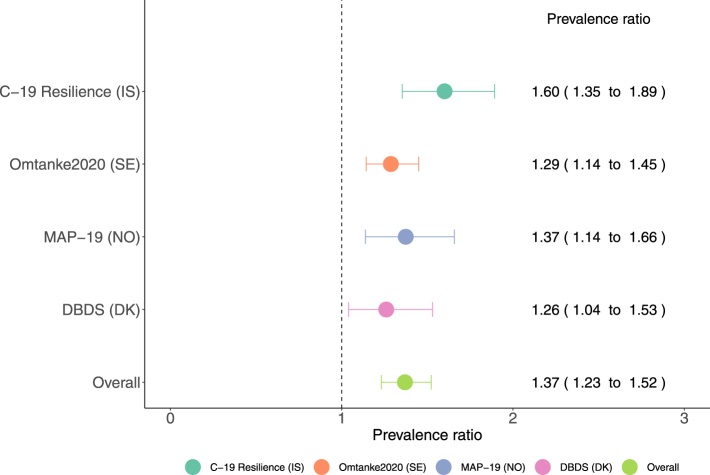
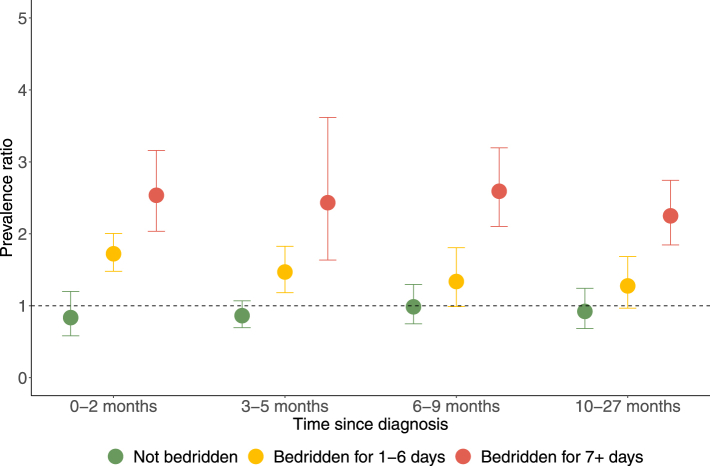
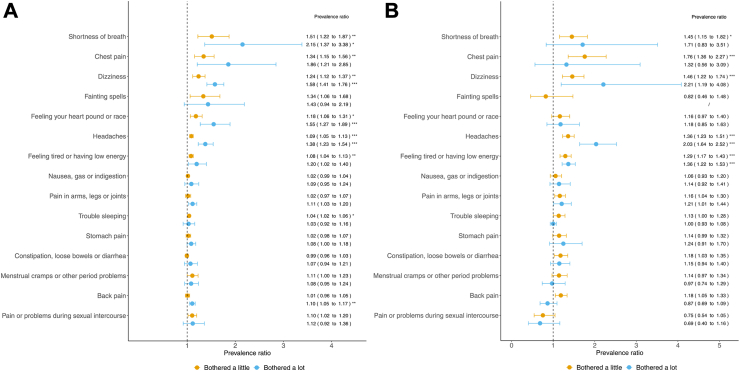
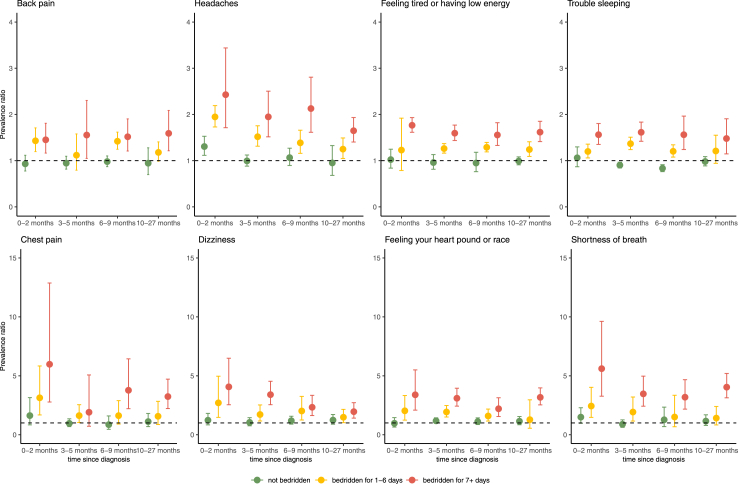
Findings: During up to 27 months of follow-up, 34.5% participants (22,382/64,880) were diagnosed with COVID-19. Individuals who were diagnosed with COVID-19, compared to those not diagnosed, had an overall 37% higher prevalence of severe physical symptom burden (PHQ-15 score ≥15, adjusted prevalence ratio [PR] 1.37 [95% confidence interval [CI] 1.23-1.52]). The prevalence was associated with acute COVID-19 severity: individuals bedridden for seven days or longer presented with the highest prevalence (PR 2.25 [1.85-2.74]), while individuals never bedridden presented with similar prevalence as individuals not diagnosed with COVID-19 (PR 0.92 [0.68-1.24]). The prevalence was statistically significantly elevated among individuals diagnosed with COVID-19 for eight of the fifteen measured symptoms: shortness of breath, chest pain, dizziness, heart racing, headaches, low energy/fatigue, trouble sleeping, and back pain. The analysis of repeated measurements rendered similar results as the main analysis.
Interpretation: These data suggest an elevated prevalence of some, but not all, physical symptoms during up to more than 2 years after diagnosis of COVID-19, particularly among individuals suffering a severe acute illness, highlighting the importance of continued monitoring and alleviation of these targeted core symptoms.
Funding: This work was mainly supported by grants from NordForsk (COVIDMENT, grant number 105668 and 138929) and Horizon 2020 (CoMorMent, 847776). See Acknowledgements for further details on funding.
Keywords: COVID-19; Cohort; Long covid; Physical symptom.
© 2023 The Author(s).
Conflict of interest statement
OAA receives support from the NordForsk (grant number 105668 COVIDMENT) and the European Union’s Horizon 2020 Research and Innovation Programme (Grant 847776; CoMorMent). OAA declares receiving grants or contracts from NIH NIMN Award (R01MH123724-01, 1R01MH124839, 1R01MH129742, 1R01MH129858-01A1), Research Council of Norway (RCN grants 223273, 296030, 300309, 324252), the South-East Norway Health Authority (grant 2017-112, 2022-073), European Union’s Horizon 2020 Research and Innovation Programme (Grant 964874 REALMENT), EEA-RO-NO-2018-0535, and KG Jebsen Stiftelsen (grants SKGJ-MED-008 and SKGJ-MED-021). OAA receives consulting fees from Biogen, Cortechs.ai and Milken. OAA gets Speaker’s honorarium from Janssen, Lundbeck and Sunovion, and has a patent on Intranasal Administration (US20160310683 A1). OAA participated in advisory board as National PI for JANSSEN trial depression, MAPS trial PTSD and BI trial schizophrenia. OAA declares having stock at Cortechs.ai. RP receives grant of Excellence, Icelandic Research Fund. RP declares to be the vice president at UEMS Section of Internal Medicine, a board member of the Icelandic Society of Internal Medicine, and is the president of the Icelandic Transplantation Society. EF received a payment for keynote lecture from Astra Zeneca. SUJ is a leader in Metacognitive Therapy Institute Norwegian Branch. FF receives support from the NordForsk (grant number 105668 and 138929 COVIDMENT) and the Horizon 2020 (Grant 847776; CoMorMent). UAV receives support from the NordForsk (grant number 105668 and 138929 COVIDMENT) and the Horizon 2020 (Grant 847776; CoMorMent). AL declares to receive Fredrik and Ingrid Thuring Foundation. OBVP receives Independent Research Fund Denmark (0214-00127B). QS declares receiving support from the Outstanding Clinical Discipline Project of Shanghai Pudong (Grant No.: PWYgy2021-02) and the Fundamental Research Funds for the Central Universities. PFS declares receiving funding from the Swedish Research Council (Vetenskapsrådet, award D0886501). PFS also receives consulting fees, participating on a data safety monitoring board or advisory board, and holds stock or stock options, from Neumora Therapeutics. All other authors declare no competing interests.
Figures
Similar articles
-
Acute COVID-19 severity and mental health morbidity trajectories in patient populations of six nations: an observational study.Lancet Public Health. 2022 May;7(5):e406-e416. doi: 10.1016/S2468-2667(22)00042-1. Epub 2022 Mar 14. Lancet Public Health. 2022. PMID: 35298894 Free PMC article.
-
Elevated symptoms of depression and anxiety among family members and friends of critically ill COVID-19 patients - an observational study of five cohorts across four countries.Lancet Reg Health Eur. 2023 Sep 4;33:100733. doi: 10.1016/j.lanepe.2023.100733. eCollection 2023 Oct. Lancet Reg Health Eur. 2023. PMID: 37953992 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Prevalence of post-acute COVID-19 syndrome symptoms at different follow-up periods: a systematic review and meta-analysis.Clin Microbiol Infect. 2022 May;28(5):657-666. doi: 10.1016/j.cmi.2022.01.014. Epub 2022 Feb 3. Clin Microbiol Infect. 2022. PMID: 35124265 Free PMC article. Review.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses.Cochrane Database Syst Rev. 2023 Jan 30;1(1):CD006207. doi: 10.1002/14651858.CD006207.pub6. Cochrane Database Syst Rev. 2023. PMID: 36715243 Free PMC article. Review.
Cited by
-
Regional geographies and public health lessons of the COVID-19 pandemic in the Arctic.Front Public Health. 2024 Jan 8;11:1324105. doi: 10.3389/fpubh.2023.1324105. eCollection 2023. Front Public Health. 2024. PMID: 38259778 Free PMC article.
-
Effects of yoga compared with health promotion on health-related quality of life in adults with post-COVID-19 condition: protocol for a randomised controlled trial.BMJ Open. 2024 Sep 12;14(9):e085525. doi: 10.1136/bmjopen-2024-085525. BMJ Open. 2024. PMID: 39266315 Free PMC article.
-
Burden of post-acute COVID-19 sequelae in healthcare workers and its course over a 30-month period-results from a prospective multicentre cohort.Infection. 2024 Nov 12. doi: 10.1007/s15010-024-02418-3. Online ahead of print. Infection. 2024. PMID: 39532773
-
Six-month follow-up of multidomain cognitive impairment in non-hospitalized individuals with post-COVID-19 syndrome.Eur Arch Psychiatry Clin Neurosci. 2024 Dec;274(8):1945-1957. doi: 10.1007/s00406-024-01863-3. Epub 2024 Jul 24. Eur Arch Psychiatry Clin Neurosci. 2024. PMID: 39048833 Free PMC article.
-
Association of physical symptoms with accelerometer-measured movement behaviors and functional capacity in individuals with Long COVID.Sci Rep. 2024 Sep 4;14(1):20652. doi: 10.1038/s41598-024-71589-8. Sci Rep. 2024. PMID: 39232125 Free PMC article.
References
-
- COVID - coronavirus statistics - Worldometer. https://www.worldometers.info/coronavirus/ [cited 2023 March 28]. Available from:
-
- Coronavirus disease (COVID-19): post COVID-19 condition. https://www.who.int/news-room/questions-and-answers/item/coronavirus-dis... [cited 2022 June 20]. Available from:
-
- Brodin P. Immune determinants of COVID-19 disease presentation and severity. Nat Med. 2021;27(1):28–33. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
