

doi: 10.1128/spectrum.03466-23.
Epub 2023 Dec 14.
Evaluation of a minimal array of Treponema pallidum antigens as biomarkers for syphilis diagnosis, infection staging, and response to treatment
Affiliations
- PMID: 38095465
- PMCID: PMC10782976
- DOI: 10.1128/spectrum.03466-23
Item in Clipboard
Evaluation of a minimal array of Treponema pallidum antigens as biomarkers for syphilis diagnosis, infection staging, and response to treatment
Microbiol Spectr.
.
Abstract
This manuscript explores the host humoral response to selected antigens of the syphilis agent during infection to evaluate their potential use as diagnostic tests and markers for treatment.
Keywords: Treponema pallidum; protein array; serodiagnosis; staging; syphilis; treatment response.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
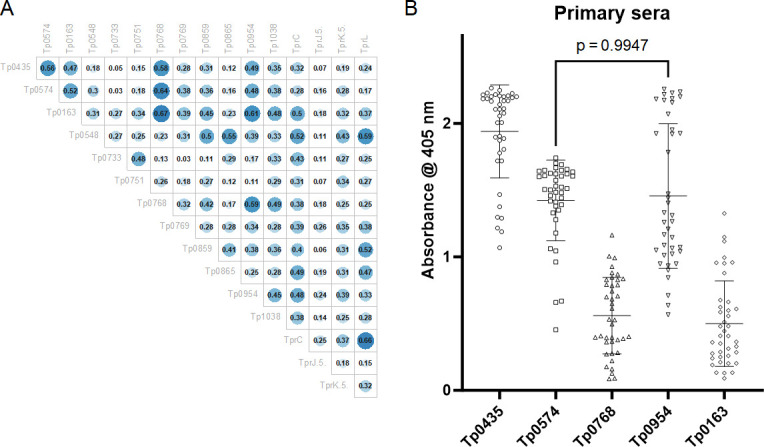
Correlation in baseline sera between immunodominant antigens and additional proteins in the array. (A) Pearson correlation coefficients showing that at baseline, Tp0163, Tp0768, and Tp0954 reactivity correlates with that of the immunodominant Tp0435 and Tp0574 antigens. A coefficient value ≥0.47 was used as the cut-off. (B) Baseline primary sera reactivity to Tp435, Tp0574, Tp0163, Tp0769, and Tp0954 plotted as individual values with mean ± standard deviation. Except for Tp0954 and Tp0574 (P = 0.99), the reactivity of Tp0163, Tp0954, and Tp0769 is significantly different from that of the immunodominant antigens.
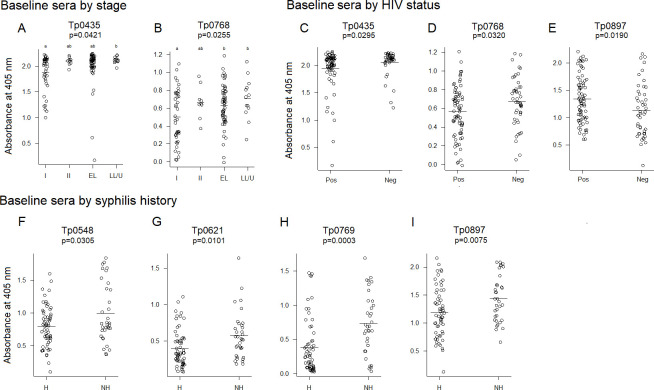
Baseline reactivity to selected T. pallidum antigens. Antigens to which a significant difference in reactivity was detected in baseline sera (collected at diagnosis and prior to treatment) using stage (A, B), HIV status (C–E), and syphilis history (F–I) as covariates. In panels (A and B), the P-value indicates that there is a significant difference across the means of the four groups analyzed. Groups lean toward statistically significant differences in means (P < 0.1) if they do not share a letter. I, primary syphilis; II, secondary syphilis; EL, early latent; LL, late latent; U: latency of unknown duration; Pos, HIV-positive patients; Neg: HIV-negative patients; H, patients with history of syphilis; NH, patients with no history of syphilis. The horizontal bar indicates the mean absorbance value. Analyses in panels (A, B) were performed with 118 samples. Analyses in panels (C–E) were performed with 120 samples. Analysis in panels (F–I) was performed with 93 samples.
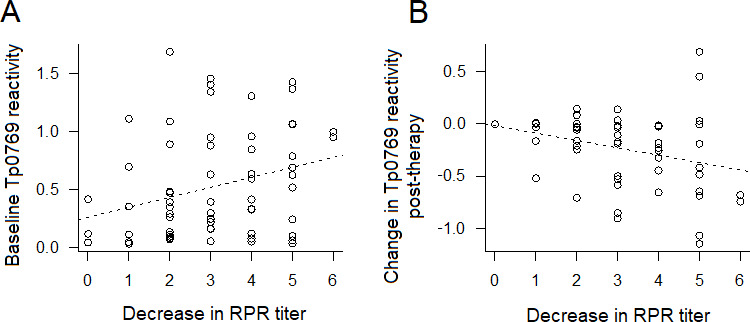
Correlation between reactivity of Tp0769 at baseline and decrease in RPR titer and between changes in Tp0769 at time point 2 (tp2) post-treatment and decrease in RPR titer. (A) Higher baseline levels of Tp0769 are associated with a higher RPR titer. Correlation P-value =0.02. (B) Decrease in Tp0769 post-treatment is associated with the decrease of RPR titer. Dotted lines represent a fitted regression model (antigen~decrease in RPR dilution). N at baseline = 64; N with change = 51. For the RPR titers, 0–6 values represent 1:1–1:64.
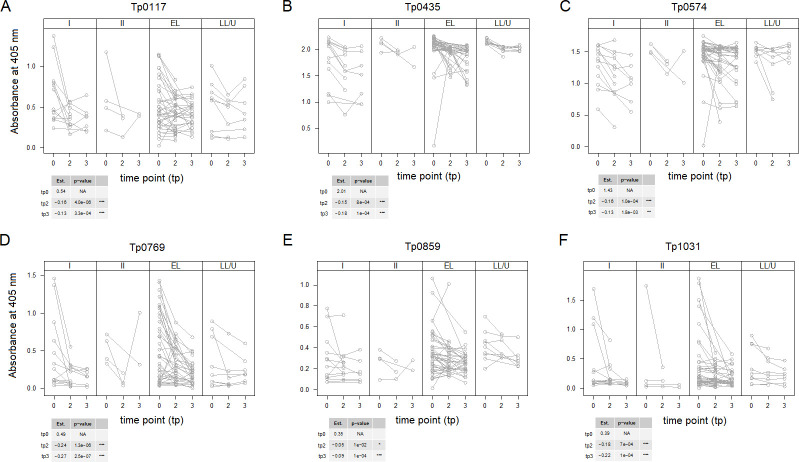
Longitudinal reactivity to selected T. pallidum antigens without considering covariates. Antigens to which sera reactivity decreased significantly post-treatment. Time points 0, 1, and 2 include baseline sera (tp0) and convalescent sera collected at 3 months [time point 2 (tp2)] and 6 months [time point 3 (tp3)] post-treatment. Values are displayed by stage to minimize overplotting. Antigens are reported in gene number order. In the tables associated to each figure panel, the “Est” column reports the mean reactivity for all samples at baseline (tp0 row) and the amount by which antigen reactivity declined at tp2 and tp3 compared to baseline. Asterisks indicate significance with Bonferroni-adjusted P-values ≤0.001 (***), ≤0.01 (**), and ≤0.05 (*). A total of 66 samples were analyzed for tp0, 51 samples for tp2, and 44 people at tp3, as not all tp3 patients provided a sample at 3 months post-treatment. The steepest declines were seen for Tp0769 (D) and Tp0117 (A).
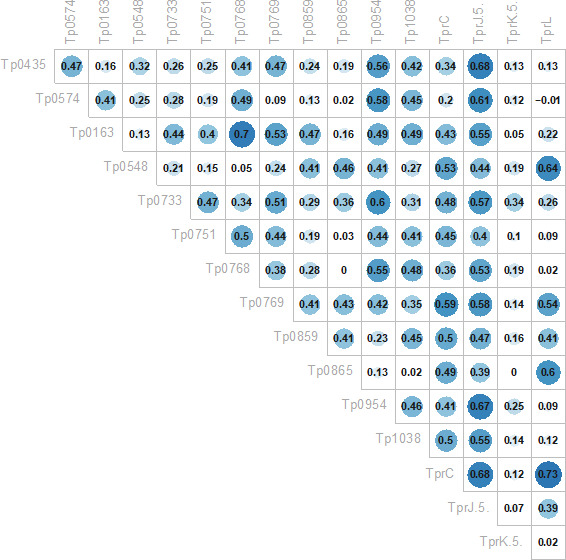
Correlation between changes in serum reactivity over time between immunodominant antigens and additional proteins in the array. Pearson correlation coefficients showing that the decrease in reactivity in Tp0769 correlates strongly with a decrease in reactivity in Tp0117/TprC, Tp0621/TprJ.5′, and Tp1031/TprL. A coefficient value ≥0.47 was used as the cut-off.
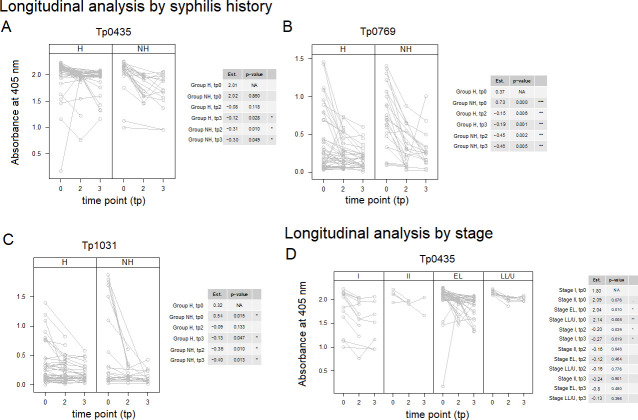
Longitudinal reactivity to selected T. pallidum antigens including covariates. Antigens to which sera reactivity decreased significantly post-treatment (Fig. 3) were further analyzed using syphilis history (A–C), stage (D), and HIV status. The models shown were significantly better than models using time alone. Time points 0, 1, and 2 include baseline sera (tp0) and convalescent sera collected at 3 (tp2) and 6 (tp3) months post-treatment. Antigens are reported in the gene number order. In the tables associated with each figure panel, the “Est” column reports the mean reactivity for samples in each group at baseline (tp0 row) and the amount by which antigen reactivity declined at tp2 and tp3 compared to baseline. Asterisks indicate significance with Bonferroni-adjusted P-values ≤0.001 (***), ≤0.01 (**), and ≤0.05 (*). No significant differences were seen when HIV status was used as a covariant. A total of 66 samples were analyzed for tp0, 51 samples for tp2, and 44 people at tp3, as not all tp3 patients provided a sample at tp2 post-treatment.
Similar articles
-
Analysis of the humoral immune response to Treponema pallidum in the different stages of untreated human syphilis.Zentralbl Bakteriol. 1989 Jul;271(2):171-9. doi: 10.1016/s0934-8840(89)80070-2. Zentralbl Bakteriol. 1989. PMID: 2673265
-
Immunochip for Syphilis Serodiagnostics with the Use of Extended Array of Treponema pallidum Recombinant Antigens.Bull Exp Biol Med. 2018 Oct;165(6):767-771. doi: 10.1007/s10517-018-4261-0. Epub 2018 Oct 23. Bull Exp Biol Med. 2018. PMID: 30353336
-
Response of Treponema pallidum particle agglutination test titers to treatment of syphilis.Clin Infect Dis. 2013 Feb;56(3):463-4. doi: 10.1093/cid/cis850. Epub 2012 Oct 5. Clin Infect Dis. 2013. PMID: 23042973 No abstract available.
-
Novel Treponema pallidum Recombinant Antigens for Syphilis Diagnostics: Current Status and Future Prospects.Biomed Res Int. 2017;2017:1436080. doi: 10.1155/2017/1436080. Epub 2017 Apr 24. Biomed Res Int. 2017. PMID: 28523273 Free PMC article. Review.
-
Syphilis--diagnosis and treatment.Clin Obstet Gynecol. 1975 Mar;18(1):163-82. doi: 10.1097/00003081-197503000-00015. Clin Obstet Gynecol. 1975. PMID: 1091382 Review. No abstract available.
Cited by
-
A novel pan-proteome array for high-throughput profiling of the humoral response to Treponema pallidum.iScience. 2024 Jul 31;27(9):110618. doi: 10.1016/j.isci.2024.110618. eCollection 2024 Sep 20. iScience. 2024. PMID: 39262771 Free PMC article.
-
Neurosyphilis: insights into its pathogenesis, susceptibility, diagnosis, treatment, and prevention.Front Neurol. 2024 Jan 11;14:1340321. doi: 10.3389/fneur.2023.1340321. eCollection 2023. Front Neurol. 2024. PMID: 38274871 Free PMC article. Review.
References
-
- WHO . Prevalence and incidence of selected sexually transmitted infections Chlamydia trachomatis, Neisseria gonorrhoeae, syphilis and Trichomonas vaginalis: methods and results used by WHO to generate 2005 estimates. World Health Organization, Geneva. 2011.
-
- Gerbase AC, Rowley JT, Heymann DH, Berkley SF, Piot P. 1998. Global prevalence and incidence estimates of selected curable STDs. Sex Transm Infect 74 Suppl 1:S12–6. - PubMed
-
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators . 2017. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet 390:1211–1259. doi:10.1016/S0140-6736(17)32154-2 - DOI - PMC - PubMed
-
- Newman L, Rowley J, Vander Hoorn S, Wijesooriya NS, Unemo M, Low N, Stevens G, Gottlieb S, Kiarie J, Temmerman M. 2015. Global estimates of the prevalence and incidence of four curable sexually transmitted infections in 2012 based on systematic review and global reporting. PLoS One 10:e0143304. doi:10.1371/journal.pone.0143304 - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
