

Age- and sex-stratified detection rates and associated factors of colorectal neoplasia in the Tianjin colorectal cancer screening program from 2012 to 2020
- PMID: 38087194
- PMCID: PMC10714643
- DOI: 10.1186/s12876-023-03060-3
Age- and sex-stratified detection rates and associated factors of colorectal neoplasia in the Tianjin colorectal cancer screening program from 2012 to 2020
Abstract
Purpose: Colorectal cancer (CRC) screening has been implemented in Tianjin, China since 2012. The objective was to estimate the neoplasia detection rate in a high-risk population by age and sex and to investigate the potential factors associated with colorectal neoplasia.
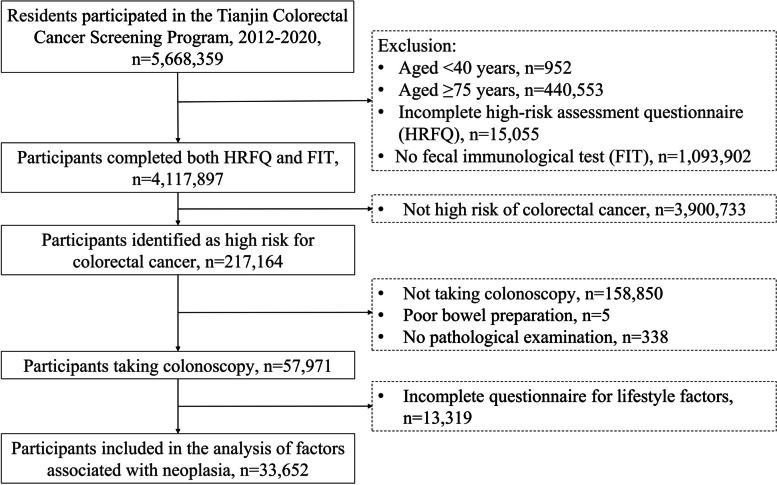
Patients and methods: This study is based on data of the Tianjin CRC screening program from 2012 to 2020. Residents with a positive high-risk factors questionnaire (HRFQ) or a positive faecal immunochemical test (FIT) were identified as high-risk participants and were subsequently recommended for a free colonoscopy.
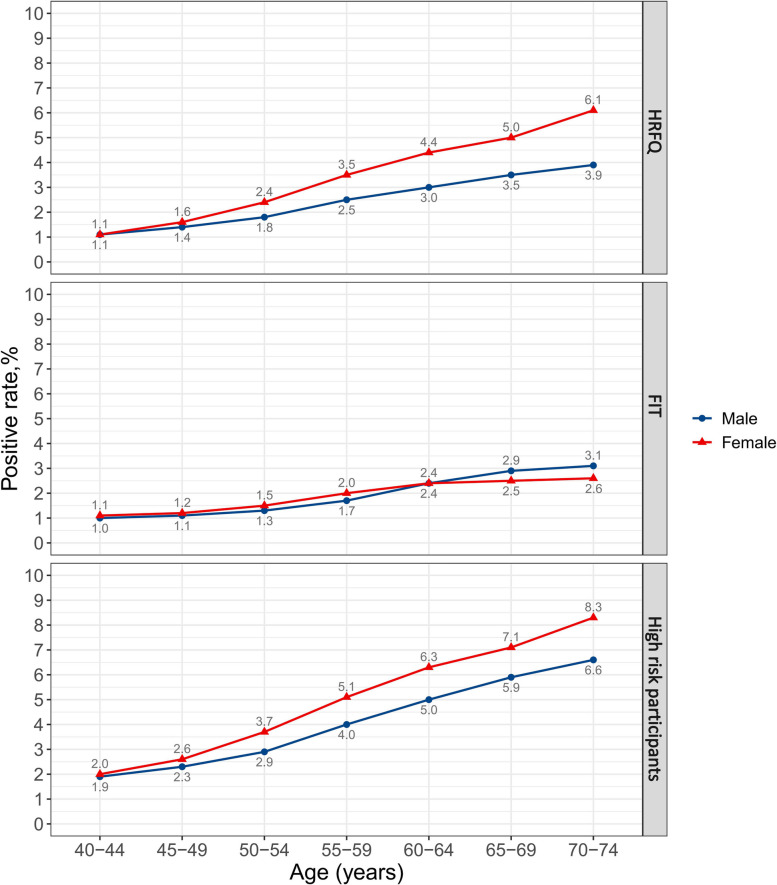
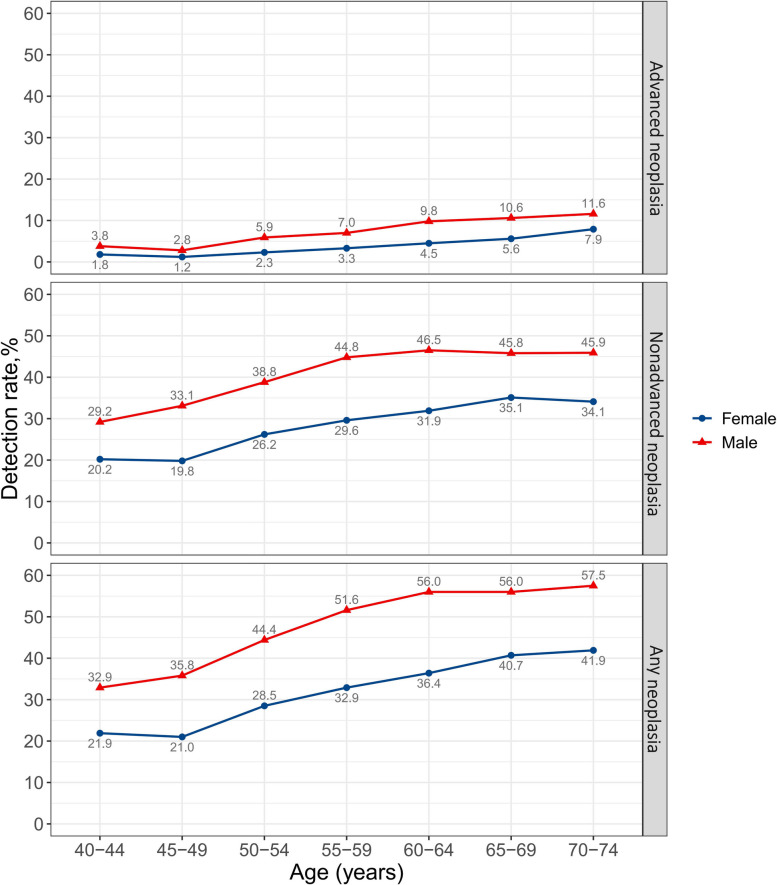
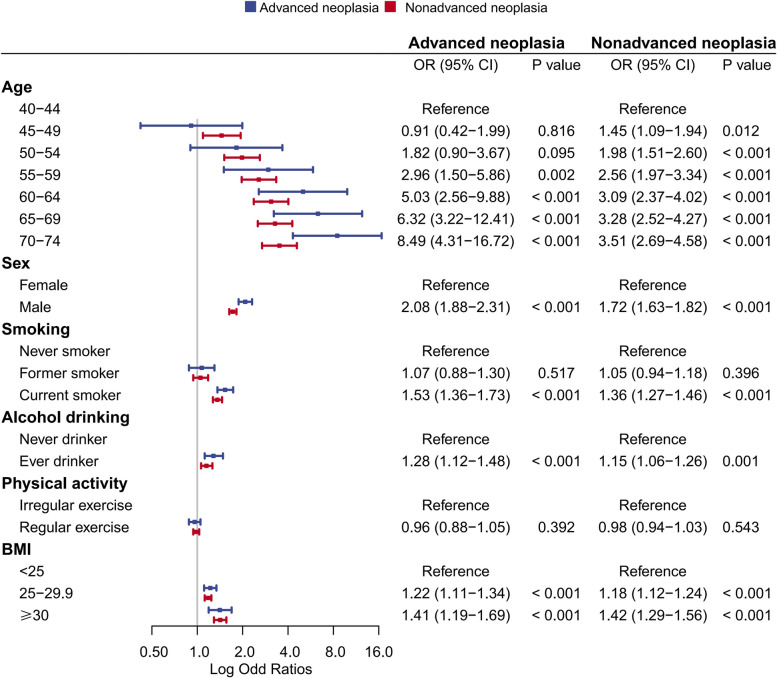
Results: A total of 4,117,897 eligible participants aged 40-74 years completed both a HRFQ and FIT, and 217,164 (5.3%) of them were identified as high-risk participants. Positive rates of preliminary screening increased with age and were higher in females than in males. For 57,971 participants undertaking colonoscopy, the detection rates of nonadvanced adenoma, advanced adenoma and CRC were 37.8%, 5.7% and 1.6%, respectively. Detection rates of advanced neoplasia increased from the age of 50 and were higher in males. For nonadvanced neoplasia, a strong increase was observed in males from the age of 40 and in females from the age of 50. Male sex had a greater impact on individuals aged 40-49 than on older individuals. Several factors including current smoking, drinking, and higher body mass index (BMI) were significantly associated with the presence of neoplasia, whereas, these associations were mainly restricted to individuals aged above 50 but not those aged 40-49 years.
Conclusions: These findings support that age-specific risk stratification and sex-specific initiating ages for CRC screening should be recommended to improve the accuracy and effectiveness of current screening strategy.
Keywords: CRC screening; Cancer prevention; Early-onset CRC; Risk factors.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
[Efficacy comparison among high risk factors questionnaire and Asia-Pacific colorectal screening score and their combinations with fecal immunochemical test in screening advanced colorectal tumor].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Jul 25;25(7):612-620. doi: 10.3760/cma.j.cn441530-20211127-00478. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35844124 Chinese.
-
Postponing colonoscopy for 6 months in high-risk population increases colorectal cancer detection in China.Cancer Med. 2023 May;12(10):11816-11827. doi: 10.1002/cam4.5850. Epub 2023 Mar 23. Cancer Med. 2023. PMID: 36951442 Free PMC article.
-
Combining FITs and HRFQ with colonoscopy improve the cost-effectiveness of a 9-year mass colorectal cancer screening program.ESMO Open. 2024 Sep;9(9):103676. doi: 10.1016/j.esmoop.2024.103676. Epub 2024 Aug 20. ESMO Open. 2024. PMID: 39168026 Free PMC article.
-
How significant is the association between metabolic syndrome and prevalence of colorectal neoplasia?World J Gastroenterol. 2016 Sep 28;22(36):8103-11. doi: 10.3748/wjg.v22.i36.8103. World J Gastroenterol. 2016. PMID: 27688652 Free PMC article. Review.
-
Colorectal Cancer Risk Assessment and Precision Approaches to Screening: Brave New World or Worlds Apart?Gastroenterology. 2023 Apr;164(5):812-827. doi: 10.1053/j.gastro.2023.02.021. Epub 2023 Feb 24. Gastroenterology. 2023. PMID: 36841490 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
