

Interdisciplinary aspects of abdominal and plastic surgery - what does the (abdominal) surgeon need to know?
- PMID: 38058780
- PMCID: PMC10696945
- DOI: 10.1515/iss-2023-0042
Interdisciplinary aspects of abdominal and plastic surgery - what does the (abdominal) surgeon need to know?
Abstract
Introduction: The aim was to reflect the established interdisciplinary aspects of general/abdominal and plastic surgery by means of a narrative review. Methods: (i) With specific references out of the medical literature and (ii) own clinical and perioperative as well as operating technical and tactical management experiences obtained in surgical daily practice, we present a choice of options for interdisciplinary cooperation that could be food of thought for other surgeons.
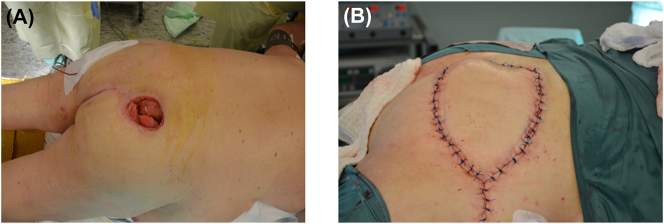
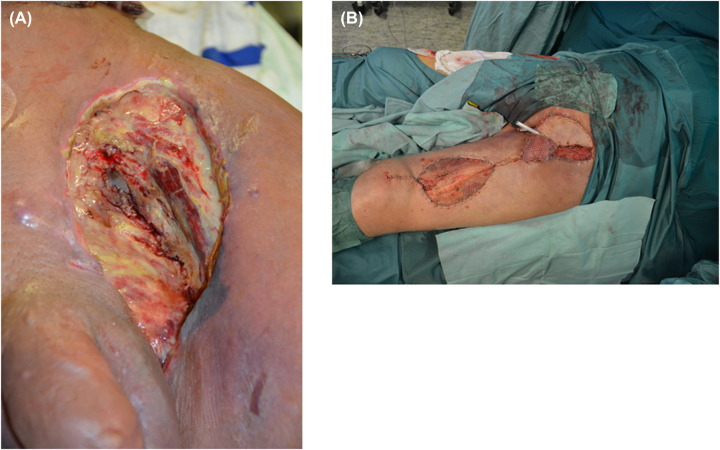
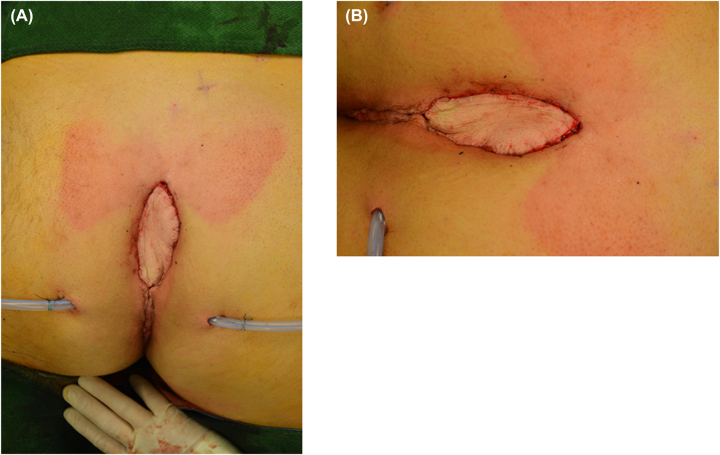
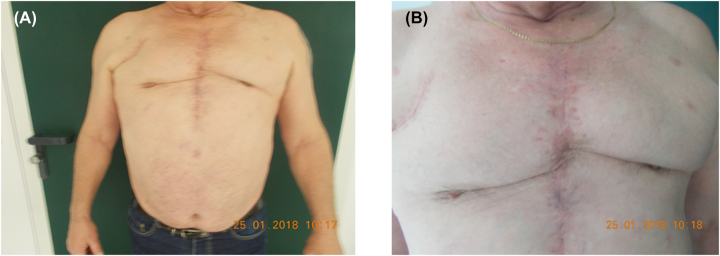
Content: - Decubital ulcers require pressure relieve, debridement and plastic surgery coverage, e.g., by a rotation flap plasty, V-Y flap or "tensor-fascia-lata" (TFL) flap depending on localization (sacral/gluteal defects, ischiadic tuber). - Coverage of soft tissue defects, e.g., after lymph node dissection, tumor lesions or disturbance of wound healing can be managed with fasciocutaneous or muscle flaps. - Bariatric surgery: Surgical interventions such as butt lift, tummy tuck should be explained and demonstrated in advance and performed commonly after reduction of the body weight. - Abdominoperineal rectum extirpation (APE): Holm's procedure with greater circumferential extent of resection at the mesorectum and the insertion site of the levator muscle at the anal sphicter muscle resulting in a substantial defect is covered by myocutaneous flap plasty. - Hernia surgery: Complicated/recurrent hernias or abdominal wall defect can be covered by flap plasty to achieve functional reconstruction, e.g., using innervated muscle. Thus, abdominal wall can respond better onto changes of pressure and tension. - Necrotising fasciitis: Even in case of suspicious fasciitis, an immediate radical debridement must be performed, followed by intensive care with calculated antibiotic treatment; after appropriate stabilization tissue defects can be covered by mesh graft of flap plasty. - Soft tissue tumor lesions cannot be resected with primary closure to achieve appropriate as intended R0 resection status by means of local radical resection all the time - plastic surgery expertise has to be included into interdisciplinary tumor concepts. - Liposuction/-filling: Liposuction can be used with aesthetic intention after bariatric surgery or for lipedema. Lipofilling is possible for reconstruction and for aesthetic purpose. - Reconstruction of lymphatic vessels: Lymphedema after tumor operations interrupting or blocking lymphatic drainage can be treated with microsurgical reconstructions (such as lympho-venous anastomoses, lympho-lymphatic anastomoses or free microvascular lymph node transfer). - Microsurgery: It is substantial part of modern reconstructive plastic surgery, i.e., surgery of peripheral nerves belongs to this field. For visceral surgery, it can become important for reconstruction of the recurrent laryngeal nerve. - Sternum osteomyelitis: Radical debridement (eventually, complete sternal resection) with conditioning of the wound by vacuum-assisted closure followed by plastic surgery coverage can prevent chronification, threatening mediastinitis, persisting infectious risk, long-term suffering or limited quality of life.
Summary: The presented selection of single topics can only be an excerpt of all the options for surgical cooperation in daily clinical and surgical practice.
Outlook: An interdisciplinary approach of abdominal and plastic surgery is characterized by a highly developed cooperation in common surgical interventions including various techniques and tactics highlighting the specifics of the two fields.
Keywords: abdominal surgery; latissimus-dorsi flap; pediculated/free flap transfer; plastic surgery; rectus-abdominis flap.
© 2023 the author(s), published by De Gruyter, Berlin/Boston.
Conflict of interest statement
Competing interests: Authors state no conflict of interest.
Figures

Similar articles
-
What does a (general and abdominal) surgeon need to know on plastic surgery?Pol Przegl Chir. 2019 Jun 6;91(5):41-50. doi: 10.5604/01.3001.0013.2365. Pol Przegl Chir. 2019. PMID: 31702575
-
Free innervated latissimus dorsi muscle flap for reconstruction of full-thickness abdominal wall defects.Plast Reconstr Surg. 1998 Apr;101(4):971-8. doi: 10.1097/00006534-199804040-00013. Plast Reconstr Surg. 1998. PMID: 9514329
-
The use of tensor fascia lata pedicled flap in reconstructing full thickness abdominal wall defects and groin defects following tumor ablation.J Egypt Natl Canc Inst. 2005 Sep;17(3):139-48. J Egypt Natl Canc Inst. 2005. PMID: 16799651
-
Flap technology for reconstructions of urogenital organs.Curr Opin Urol. 2003 Nov;13(6):483-8. doi: 10.1097/01.mou.0000098071.73234.fe. Curr Opin Urol. 2003. PMID: 14560143 Review.
-
Microvascular reconstruction of the breast.Semin Surg Oncol. 2000 Oct-Nov;19(3):264-71. doi: 10.1002/1098-2388(200010/11)19:3<264::aid-ssu8>3.0.co;2-d. Semin Surg Oncol. 2000. PMID: 11135483 Review.
Cited by
-
Two laterally based scrotal pedicled flap grafts in the treatment of penile skin necrosis due to ring incarceration: a case series.Sex Med. 2024 May 28;12(2):qfae030. doi: 10.1093/sexmed/qfae030. eCollection 2024 Apr. Sex Med. 2024. PMID: 38808310 Free PMC article.
References
-
- Middelberg TRBJ. Chirurgische Konzepte zur Dekubitusbehandlung: Surgical therapy concepts for the pressure sore treatment. GMS Hygiene and Infection Control. 2006;1:22.
-
- Warbanow K, Krause-Bergmann A, Berger A, Brenner P, Reichert B. Myokutane Lappen als sichere Defektdeckung bei höhergradigen pelvinen Dekubitalulzera Einteilung, Therapiekonzept und Darstellung des eigenen Krankenguts aus 16 Jahren. Langenbecks Arch Surg. 1997;382:359–66. doi: 10.1007/BF02386623. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous