

Care pathways of sepsis survivors: sequelae, mortality and use of healthcare services in France, 2015-2018
- PMID: 37950254
- PMCID: PMC10638811
- DOI: 10.1186/s13054-023-04726-w
Care pathways of sepsis survivors: sequelae, mortality and use of healthcare services in France, 2015-2018
Abstract
Background: Individuals who survive sepsis are at high risk of chronic sequelae, resulting in significant health-economic costs. Several studies have focused on aspects of healthcare pathways of sepsis survivors but comprehensive, longitudinal overview of their pathways of care are scarce. The aim of this retrospective, longitudinal cohort study is to identify sepsis survivor profiles based on their healthcare pathways and describe their healthcare consumption and costs over the 3 years following their index hospitalization.
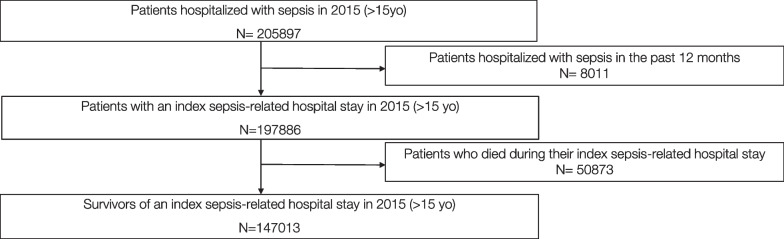
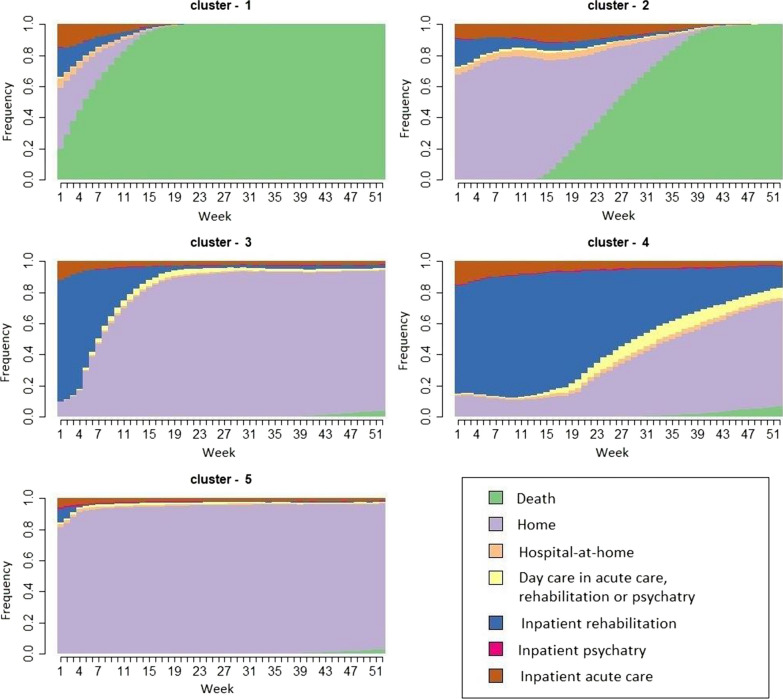
Methods: The data were extracted from the French National Hospital Discharge Database. The study population included all patients above 15 years old, with bacterial sepsis, who survived an incident hospitalization in an acute care facility in 2015. To identify survivor profiles, state sequence and clustering analyses were conducted over the year following the index hospitalization. For each profile, patient characteristics and their index hospital stay and sequelae were described, as well as use of care and its associated monetary costs, both pre- and post-sepsis.
Results: New medical (79.2%), psychological (26.9%) and cognitive (18.5%) impairments were identified post-sepsis, and 65.3% of survivors were rehospitalized in acute care. Cumulative mortality reached 36.6% by 3 years post-sepsis. The total medical cost increased by 856 million € in the year post-sepsis. Five patient clusters were identified: home (65.6% of patients), early death (12.9%), late death (6.8%), short-term rehabilitation (11.3%) and long-term rehabilitation (3.3%). Survivors with early and late death clusters had high rates of cancer and primary bacteremia and experienced more hospital-at-home care post-sepsis. Survivors in short- or long-term rehabilitation clusters were older, with higher percentage of septic shock than those coming back home, and had high rates of multiple site infections and higher rates of new psychological and cognitive impairment.
Conclusions: Over three years post-sepsis, different profiles of sepsis survivors were identified with different mortality rates, sequels and healthcare services usage and cost. This study confirmed the importance of sepsis burden and suggests that strategies of post-discharge care, in accordance with patient profile, should be further tested in order to reduce sepsis burden.
Keywords: Acute care; Healthcare pathway; Infection; Intensive care unit; Medical administrative database; Post-discharge; Rehabilitation; Sepsis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Long-term mortality and outcome in hospital survivors of septic shock, sepsis, and severe infections: The importance of aftercare.PLoS One. 2020 Feb 12;15(2):e0228952. doi: 10.1371/journal.pone.0228952. eCollection 2020. PLoS One. 2020. PMID: 32050005 Free PMC article.
-
The Effects of Postacute Rehabilitation on Mortality, Chronic Care Dependency, Health Care Use, and Costs in Sepsis Survivors.Ann Am Thorac Soc. 2023 Feb;20(2):279-288. doi: 10.1513/AnnalsATS.202203-195OC. Ann Am Thorac Soc. 2023. PMID: 36251451
-
Epidemiology and Costs of Postsepsis Morbidity, Nursing Care Dependency, and Mortality in Germany, 2013 to 2017.JAMA Netw Open. 2021 Nov 1;4(11):e2134290. doi: 10.1001/jamanetworkopen.2021.34290. JAMA Netw Open. 2021. PMID: 34767025 Free PMC article.
-
Comparing Recovery Options for Stroke Patients [Internet].Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2019 Mar. Washington (DC): Patient-Centered Outcomes Research Institute (PCORI); 2019 Mar. PMID: 37851843 Free Books & Documents. Review.
-
A systematic review of the impact of intensive care admissions on post discharge cognition in children.Eur J Pediatr. 2021 Dec;180(12):3443-3454. doi: 10.1007/s00431-021-04145-5. Epub 2021 Jun 11. Eur J Pediatr. 2021. PMID: 34114079 Free PMC article. Review.
Cited by
-
Post-discharge functional outcomes in older patients with sepsis.Crit Care. 2024 Aug 29;28(1):281. doi: 10.1186/s13054-024-05080-1. Crit Care. 2024. PMID: 39210369 Free PMC article.
-
Immunotherapy in the context of sepsis-induced immunological dysregulation.Front Immunol. 2024 May 21;15:1391395. doi: 10.3389/fimmu.2024.1391395. eCollection 2024. Front Immunol. 2024. PMID: 38835773 Free PMC article. Review.
-
Screening and Application of DNA Aptamers for Heparin-Binding Protein.Molecules. 2024 Apr 10;29(8):1717. doi: 10.3390/molecules29081717. Molecules. 2024. PMID: 38675537 Free PMC article.
References
-
- WHO. WHA70.7, Agenda item 12.2. Improving the prevention, diagnosis and clinical management of sepsis. Published online May 29, 2017.
-
- Pandolfi F, Guillemot D, Watier L, Brun-Buisson C. Trends in bacterial sepsis incidence and mortality in France between 2015 and 2019 based on National Health Data System (Système National des données de Santé (SNDS)): a retrospective observational study. BMJ Open. 2022;12(5):e058205. doi: 10.1136/bmjopen-2021-058205. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
