

Integrative multi-omics analysis unveils stemness-associated molecular subtypes in prostate cancer and pan-cancer: prognostic and therapeutic significance
- PMID: 37936202
- PMCID: PMC10629187
- DOI: 10.1186/s12967-023-04683-6
Integrative multi-omics analysis unveils stemness-associated molecular subtypes in prostate cancer and pan-cancer: prognostic and therapeutic significance
Abstract
Background: Prostate cancer (PCA) is the fifth leading cause of cancer-related deaths worldwide, with limited treatment options in the advanced stages. The immunosuppressive tumor microenvironment (TME) of PCA results in lower sensitivity to immunotherapy. Although molecular subtyping is expected to offer important clues for precision treatment of PCA, there is currently a shortage of dependable and effective molecular typing methods available for clinical practice. Therefore, we aim to propose a novel stemness-based classification approach to guide personalized clinical treatments, including immunotherapy.
Methods: An integrative multi-omics analysis of PCA was performed to evaluate stemness-level heterogeneities. Unsupervised hierarchical clustering was used to classify PCAs based on stemness signature genes. To make stemness-based patient classification more clinically applicable, a stemness subtype predictor was jointly developed by using four PCA datasets and 76 machine learning algorithms.
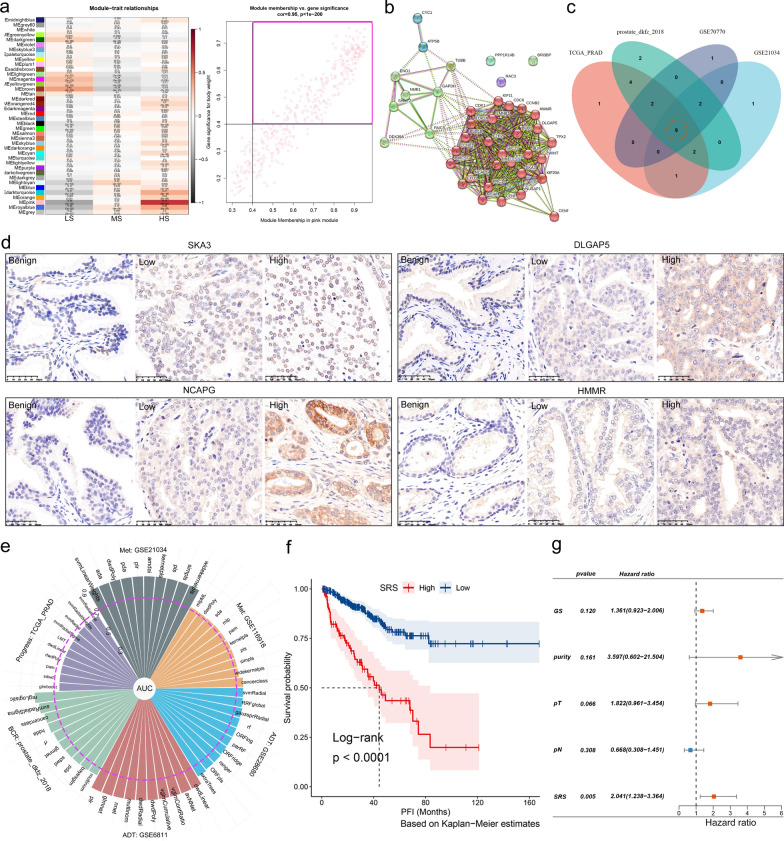
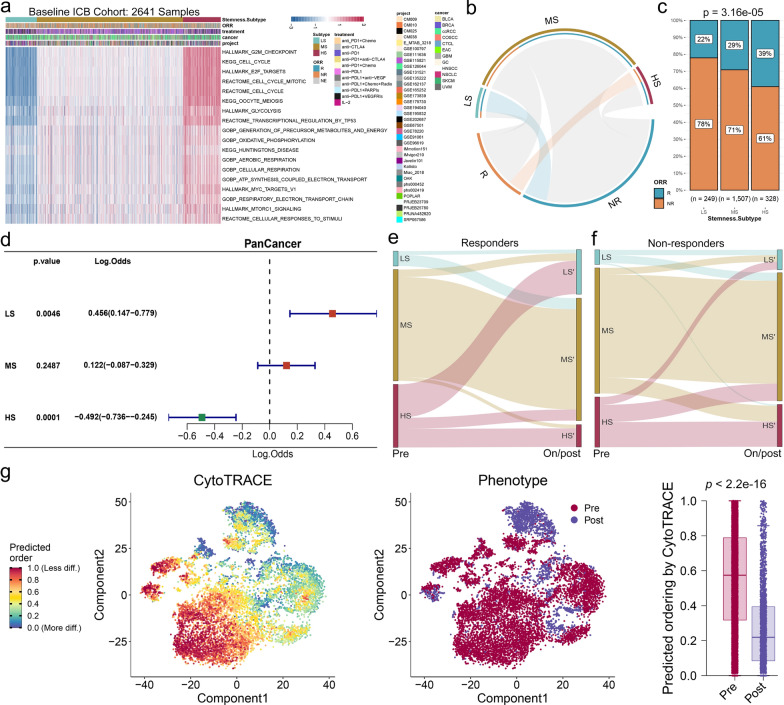
Results: We identified stemness signatures of PCA comprising 18 signaling pathways, by which we classified PCA samples into three stemness subtypes via unsupervised hierarchical clustering: low stemness (LS), medium stemness (MS), and high stemness (HS) subtypes. HS patients are sensitive to androgen deprivation therapy, taxanes, and immunotherapy and have the highest stemness, malignancy, tumor mutation load (TMB) levels, worst prognosis, and immunosuppression. LS patients are sensitive to platinum-based chemotherapy but resistant to immunotherapy and have the lowest stemness, malignancy, and TMB levels, best prognosis, and the highest immune infiltration. MS patients represent an intermediate status of stemness, malignancy, and TMB levels with a moderate prognosis. We further demonstrated that these three stemness subtypes are conserved across pan-tumor. Additionally, the 9-gene stemness subtype predictor we developed has a comparable capability to 18 signaling pathways to make tumor diagnosis and to predict tumor recurrence, metastasis, progression, prognosis, and efficacy of different treatments.
Conclusions: The three stemness subtypes we identified have the potential to be a powerful tool for clinical tumor molecular classification in PCA and pan-cancer, and to guide the selection of immunotherapy or other sensitive treatments for tumor patients.
Keywords: Immunotherapy; Machine learning; Pan‑cancer; Prostate cancer; RNA sequencing; Stemness subtype.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Figures
Similar articles
-
Tumor immune dysfunction and exclusion subtypes in bladder cancer and pan-cancer: a novel molecular subtyping strategy and immunotherapeutic prediction model.J Transl Med. 2024 Apr 17;22(1):365. doi: 10.1186/s12967-024-05186-8. J Transl Med. 2024. PMID: 38632658 Free PMC article.
-
Plasma cell subtypes analyzed using artificial intelligence algorithm for predicting biochemical recurrence, immune escape potential, and immunotherapy response of prostate cancer.Front Immunol. 2022 Dec 8;13:946209. doi: 10.3389/fimmu.2022.946209. eCollection 2022. Front Immunol. 2022. PMID: 36569837 Free PMC article.
-
Integrated machine learning identifies epithelial cell marker genes for improving outcomes and immunotherapy in prostate cancer.J Transl Med. 2023 Nov 4;21(1):782. doi: 10.1186/s12967-023-04633-2. J Transl Med. 2023. PMID: 37925432 Free PMC article.
-
The Tumor Immune Contexture of Prostate Cancer.Front Immunol. 2019 Mar 28;10:603. doi: 10.3389/fimmu.2019.00603. eCollection 2019. Front Immunol. 2019. PMID: 30984182 Free PMC article. Review.
-
The functional roles of m6A modification in prostate cancer.Proteomics Clin Appl. 2023 Nov;17(6):e2200108. doi: 10.1002/prca.202200108. Epub 2023 Oct 13. Proteomics Clin Appl. 2023. PMID: 37070355 Review.
Cited by
-
Metastatic hormone-naïve prostate cancer: a distinct biological entity.Trends Cancer. 2024 Sep;10(9):825-841. doi: 10.1016/j.trecan.2024.06.005. Epub 2024 Jul 23. Trends Cancer. 2024. PMID: 39048488 Free PMC article. Review.
-
Themis: advancing precision oncology through comprehensive molecular subtyping and optimization.Brief Bioinform. 2024 May 23;25(4):bbae261. doi: 10.1093/bib/bbae261. Brief Bioinform. 2024. PMID: 38833322 Free PMC article.
-
Contemporary Update on Clinical and Experimental Prostate Cancer Biomarkers: A Multi-Omics-Focused Approach to Detection and Risk Stratification.Biology (Basel). 2024 Sep 25;13(10):762. doi: 10.3390/biology13100762. Biology (Basel). 2024. PMID: 39452071 Free PMC article. Review.
-
Microsatellite Instability-High and High Tumor Mutation Burden Frequencies in Urologic Malignancies Off-Label for Immune Checkpoint Inhibitors in Japan: A Retrospective Single-Institutional Cohort.Cureus. 2024 Sep 13;16(9):e69366. doi: 10.7759/cureus.69366. eCollection 2024 Sep. Cureus. 2024. PMID: 39398648 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
