

Effect of AT1 receptor blockade on cardiovascular outcome after cardiac arrest: an experimental study in rats
- PMID: 37880377
- PMCID: PMC10600238
- DOI: 10.1038/s41598-023-45568-4
Effect of AT1 receptor blockade on cardiovascular outcome after cardiac arrest: an experimental study in rats
Abstract
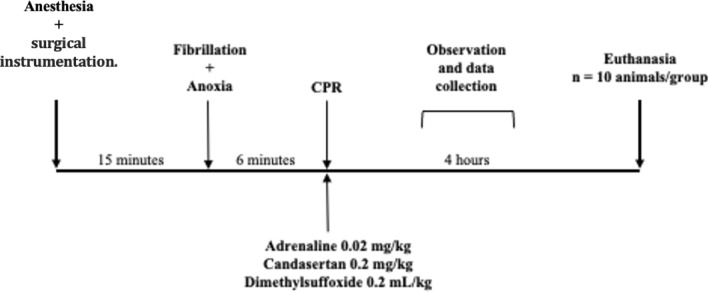
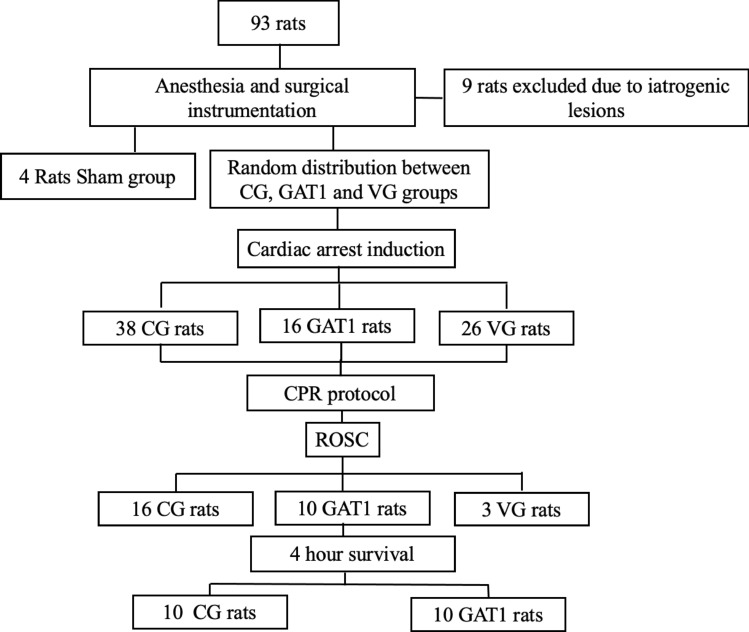
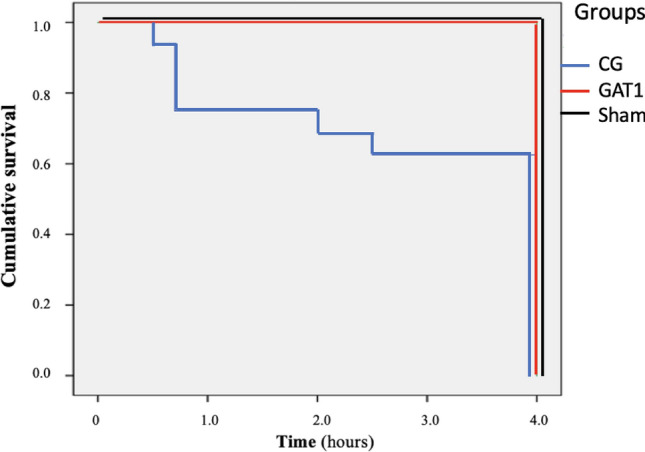
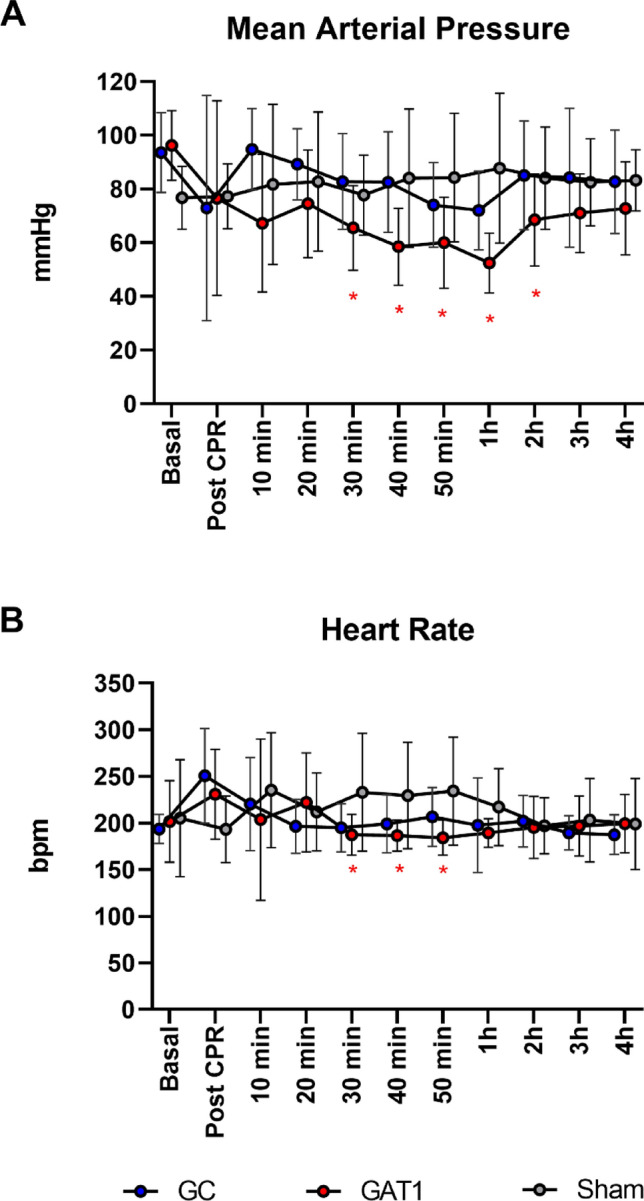
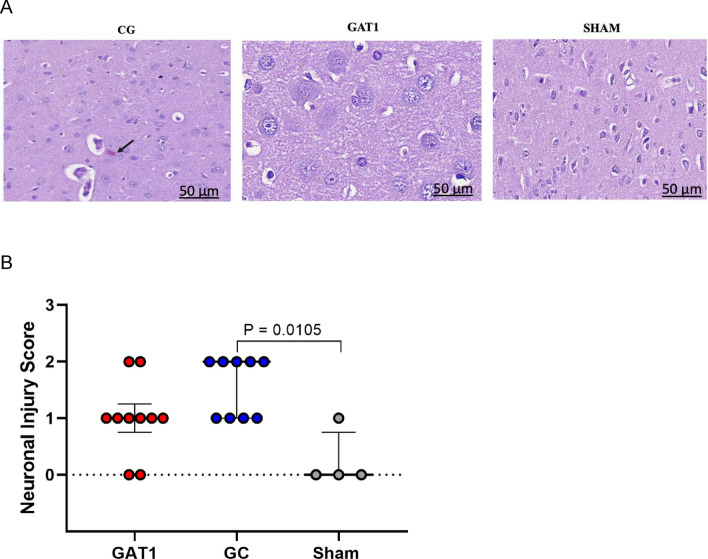
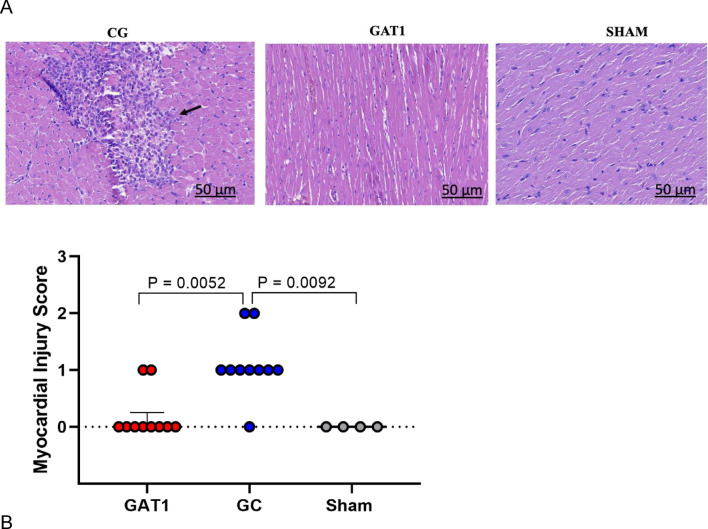
Angiotensin II receptor 1(AT1) antagonists are beneficial in focal ischemia/reperfusion (I/R). However, in cases of global I/R, such as cardiac arrest (CA), AT1 blocker's potential benefits are still unknown. Wistar male rats were allocated into four groups: Control group (CG)-animals submitted to CA by ventricular fibrillation induced by direct electrical stimulation for 3 min, and anoxia for 5 min; Group AT1 (GAT1)-animals subjected to CA and treated with 0.2 mg/kg of candesartan diluted in dimethylsulfoxide (DMSO) (0.1%); Vehicle Group (VG): animals subjected to CA and treated with 0.2 ml/kg of DMSO and Sham group (SG)-animals submitted to surgical interventions, without CA. Cardiopulmonary resuscitation consisted of group medications, chest compressions, ventilation, epinephrine (20 mcg/kg) and defibrillation. The animals were observed up to 4 h after spontaneous circulation (ROSC) return, and survival rates, hemodynamic variables, histopathology, and markers of tissue injury were analyzed. GAT1 group had a higher rate of ROSC (62.5% vs. 42.1%, p < 0.0001), survival (100% vs. 62.5%, p = 0.027), lower incidence of arrhythmia after 10 min of ROSC (10% vs. 62.5%, p = 0.000), and lower neuronal and cardiac injury scores on histology evaluation (p = 0.025 and p = 0.0052, respectively) than GC group. The groups did not differ regarding CA duration, number of adrenaline doses, or number of defibrillations. AT1 receptor blockade with candesartan yielded higher rates of ROSC and survival, in addition to neuronal and myocardial protection.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Methylene blue as an adjuvant during cardiopulmonary resuscitation: an experimental study in rats.Braz J Anesthesiol. 2024 Mar-Apr;74(2):744470. doi: 10.1016/j.bjane.2023.10.003. Epub 2023 Nov 4. Braz J Anesthesiol. 2024. PMID: 37926365 Free PMC article.
-
Erythropoietin alleviates post-resuscitation myocardial dysfunction in rats potentially through increasing the expression of angiotensin II receptor type 2 in myocardial tissues.Mol Med Rep. 2018 Apr;17(4):5184-5192. doi: 10.3892/mmr.2018.8473. Epub 2018 Jan 24. Mol Med Rep. 2018. PMID: 29393490 Free PMC article.
-
Effect of different resuscitation strategies on post-resuscitation brain damage in a porcine model of prolonged cardiac arrest.Chin Med J (Engl). 2014;127(19):3432-7. Chin Med J (Engl). 2014. PMID: 25269909
-
Effect of nitric oxide synthase modulation on resuscitation success in a swine ventricular fibrillation cardiac arrest model.Resuscitation. 2005 Oct;67(1):127-34. doi: 10.1016/j.resuscitation.2005.03.015. Epub 2005 Jul 20. Resuscitation. 2005. PMID: 16039037
-
Extracorporeal membrane oxygenation mitigates myocardial injury and improves survival in porcine model of ventricular fibrillation cardiac arrest.Scand J Trauma Resusc Emerg Med. 2019 Aug 28;27(1):82. doi: 10.1186/s13049-019-0653-z. Scand J Trauma Resusc Emerg Med. 2019. PMID: 31462264 Free PMC article.
References
-
- Vane MF, Carmona MJC, Auler JOC. Predictors and their prognostic value for no ROSC and mortality after a non-cardiac surgery intraoperative cardiac arrest: A retrospective cohort study. Rev. Bras. Anestesiol. 2017;67(4):440–449. - PubMed
-
- Girardi LN, Barie PS. Improved survival after intraoperative cardiac arrest in noncardiac surgical patients. Arch. Surg. 1995;130:15–18. - PubMed
-
- Schneider AP, Nelson DJ, Brown DD. In-hospital cardiopulmonary resuscitation: A 30-year review. J. Am. Board Family Pract. 1993;6:91–101. - PubMed
-
- Qiu Y, Wu Y, Meng M, Luo M, Zhao H, Sun H, et al. Rosuvastatin improves myocardial and neurological outcomes after asphyxial cardiac arrest and cardiopulmonary resuscitation in rats. Biomed. Pharmacother. 2017;1(87):503–508. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
