

Slowly Progressive ANCA-associated Glomerulonephritis with Strong Mesangial MPO Deposits Following a Diagnosis of Interstitial Lung Disease
- PMID: 37722892
- PMCID: PMC11116029
- DOI: 10.2169/internalmedicine.2512-23
Slowly Progressive ANCA-associated Glomerulonephritis with Strong Mesangial MPO Deposits Following a Diagnosis of Interstitial Lung Disease
Abstract
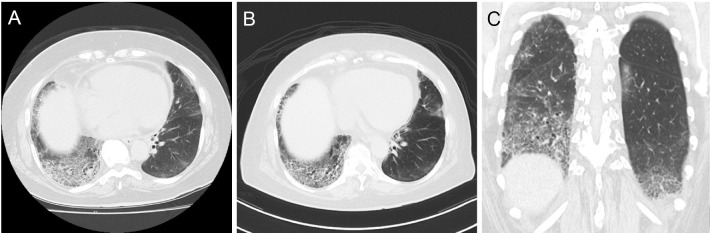
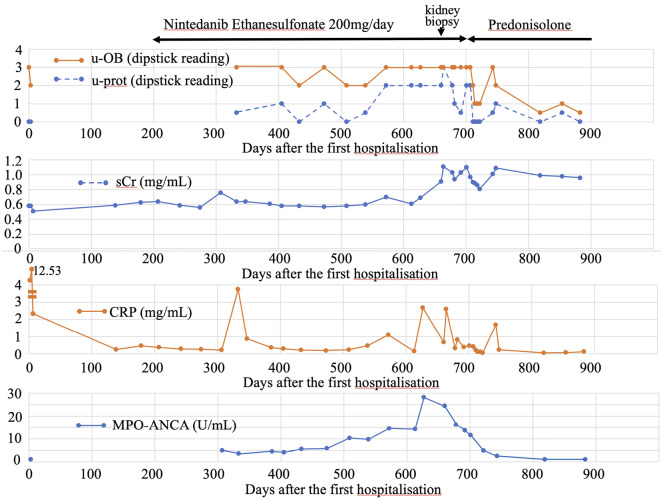
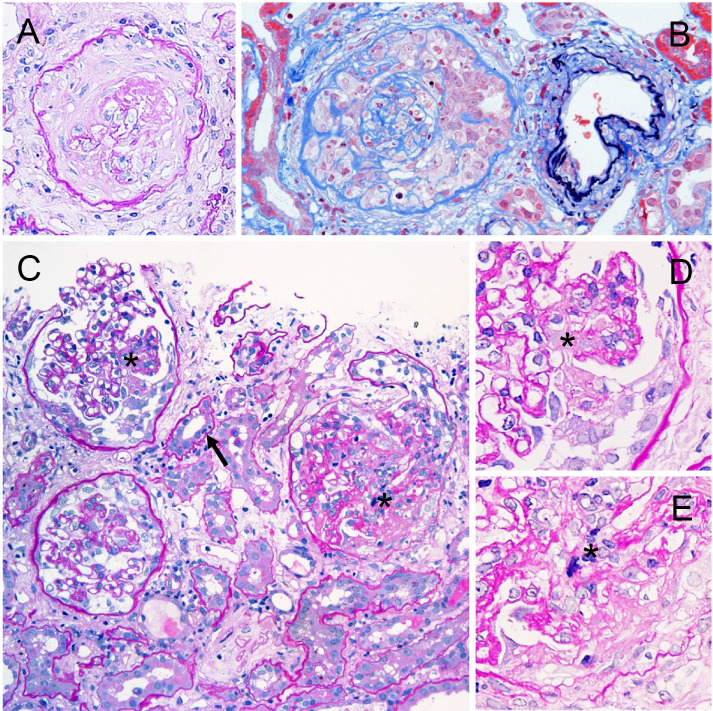
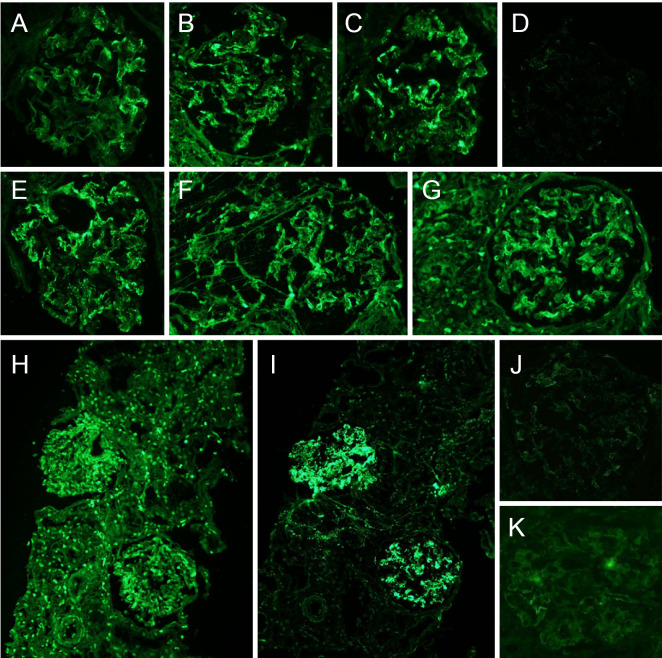
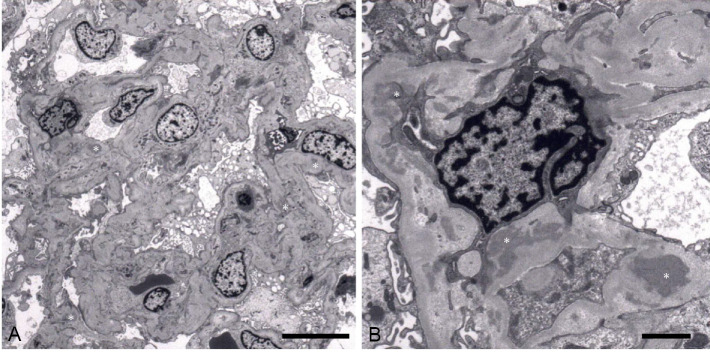
An elderly woman showed positive conversion of myeloperoxidase (MPO)-antineutrophil cytoplasmic antibodies (ANCAs) following the diagnosis of interstitial lung disease (ILD) and glomerular hematuria and subsequently experienced slowly progressive glomerulonephritis. A kidney biopsy revealed chronic damage and necrotizing crescentic glomerulonephritis with mesangial MPO deposits. After corticosteroid treatment, the patient's urinalysis results and MPO-ANCA titers almost normalized and her renal function stabilized. This case is similar to recently reported cases of slowly progressive ANCA-associated glomerulonephritis. ILD likely triggered the production of MPO-ANCAs, and the accumulation of MPO deposits in the glomeruli may have contributed to the progression of her renal disease.
Keywords: ANA; ANCA-associated glomerulonephritis; idiopathic interstitial pneumonia; myeloperoxidase.
Conflict of interest statement
Figures
Similar articles
-
ANCA-associated crescentic glomerulonephritis with mesangial IgA deposits.Am J Kidney Dis. 2000 Oct;36(4):709-18. doi: 10.1053/ajkd.2000.17615. Am J Kidney Dis. 2000. PMID: 11007672
-
[Case of MPO-ANCA positive interstitial pneumonitis and necrotizing, crescentic glomerulonephritis].Ryumachi. 1996 Dec;36(6):869-73. Ryumachi. 1996. PMID: 9122827 Japanese.
-
A pediatric occurrence of crescentic glomerulonephritis associated with antineutrophil cytoplasmic antibodies and mesangial IgA deposits.Clin Nephrol. 2007 Aug;68(2):104-8. doi: 10.5414/cnp68104. Clin Nephrol. 2007. PMID: 17722710
-
Myeloperoxidase-antineutrophil cytoplasmic antibody-associated crescentic glomerulonephritis with rheumatoid arthritis: a comparison of patients without rheumatoid arthritis.Clin Exp Nephrol. 2010 Aug;14(4):325-32. doi: 10.1007/s10157-010-0278-z. Epub 2010 Mar 26. Clin Exp Nephrol. 2010. PMID: 20339893 Review.
-
The role of myeloperoxidase and myeloperoxidase-antineutrophil cytoplasmic antibodies (MPO-ANCAs) in the pathogenesis of human MPO-ANCA-associated glomerulonephritis.Clin Exp Nephrol. 2013 Oct;17(5):634-637. doi: 10.1007/s10157-013-0787-7. Epub 2013 Mar 16. Clin Exp Nephrol. 2013. PMID: 23504409 Free PMC article. Review.
References
-
- Jennette JC. Rapidly progressive crescentic glomerulonephritis. Kidney Int 63: 1164-1177, 2003. - PubMed
-
- Haas M, Eustace JA. Immune complex deposits in ANCA-associated crescentic glomerulonephritis: a study of 126 cases. Kidney Int 65: 2145-2152, 2004. - PubMed
-
- Hirose O, Itabashi M, Takei T, Honda K, Nitta K. Antineutrophil cytoplasmic antibody-associated glomerulonephritis with immunoglobulin deposition. Clin Exp Nephrol 21: 643-650, 2017. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous