

The Oncology Biomarker Discovery framework reveals cetuximab and bevacizumab response patterns in metastatic colorectal cancer
- PMID: 37666855
- PMCID: PMC10477267
- DOI: 10.1038/s41467-023-41011-4
The Oncology Biomarker Discovery framework reveals cetuximab and bevacizumab response patterns in metastatic colorectal cancer
Abstract
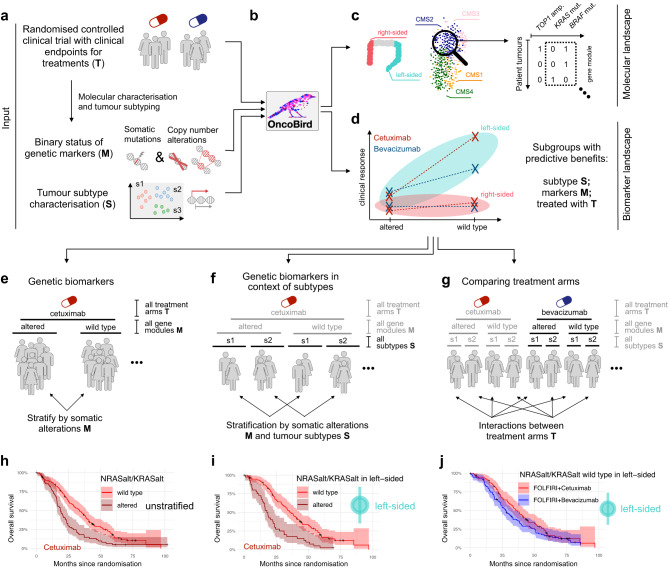
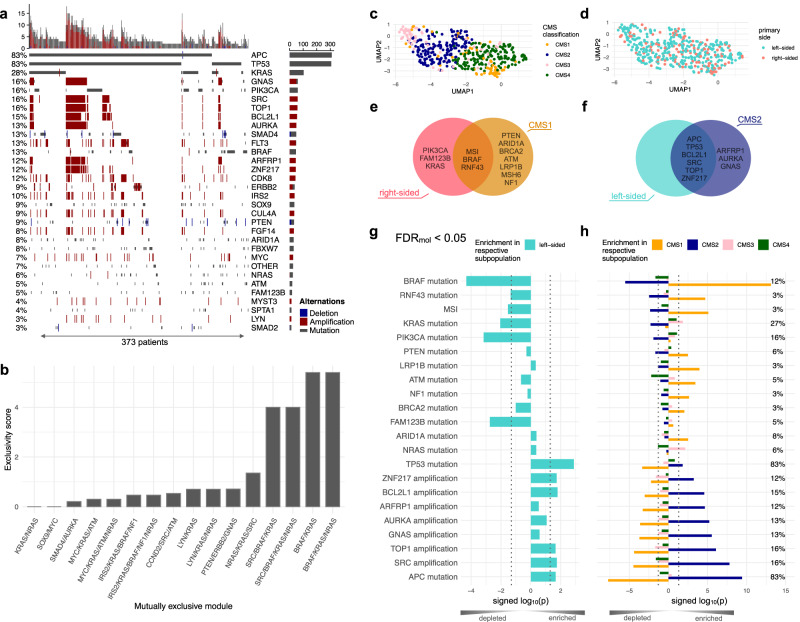
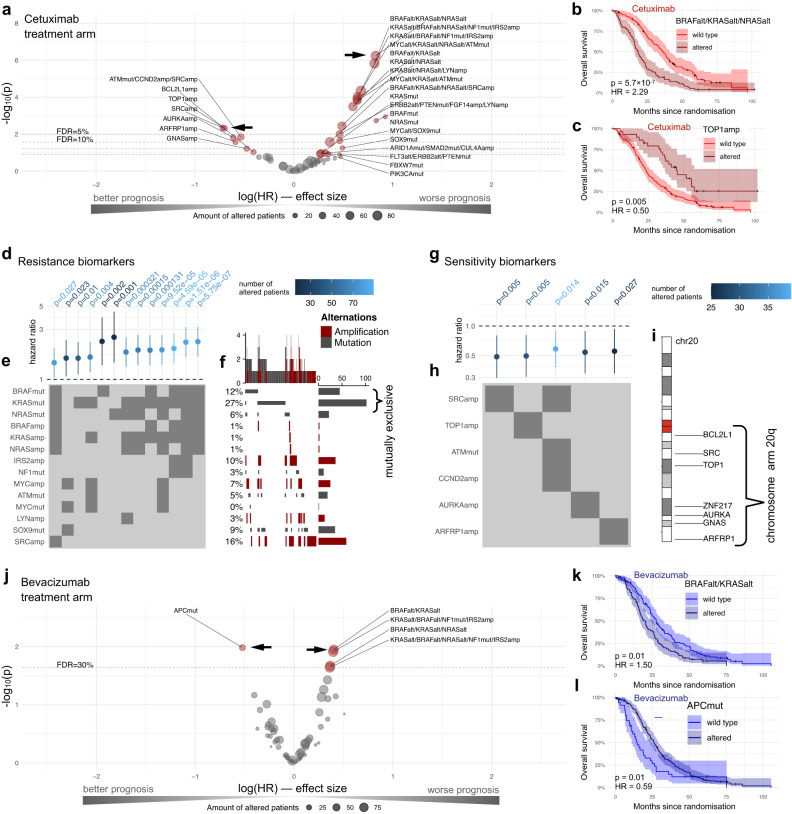
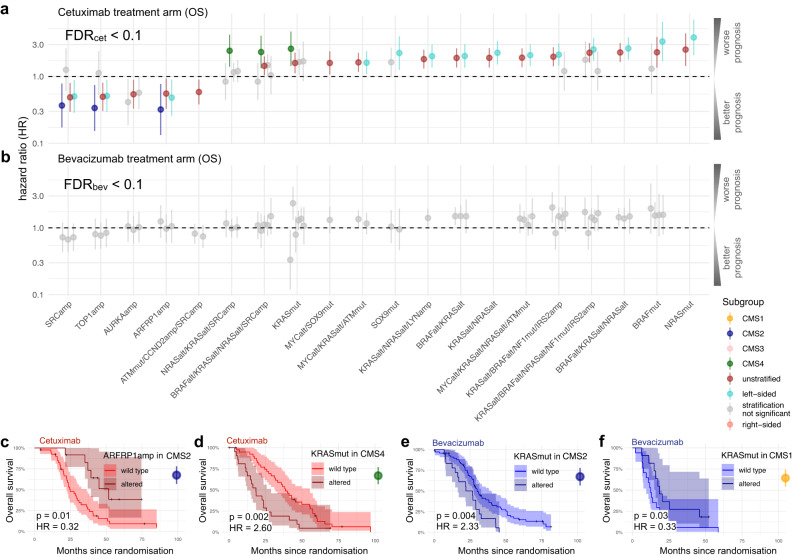
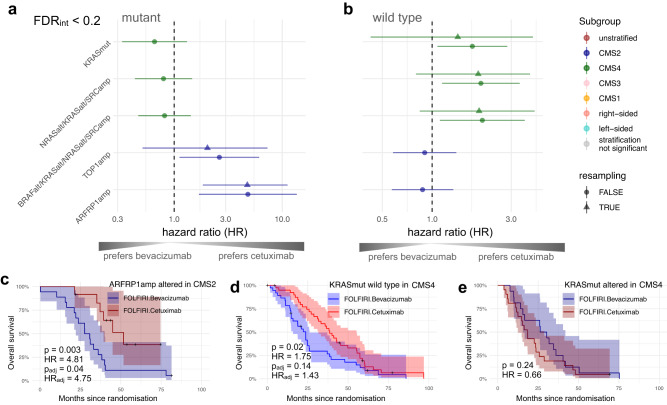
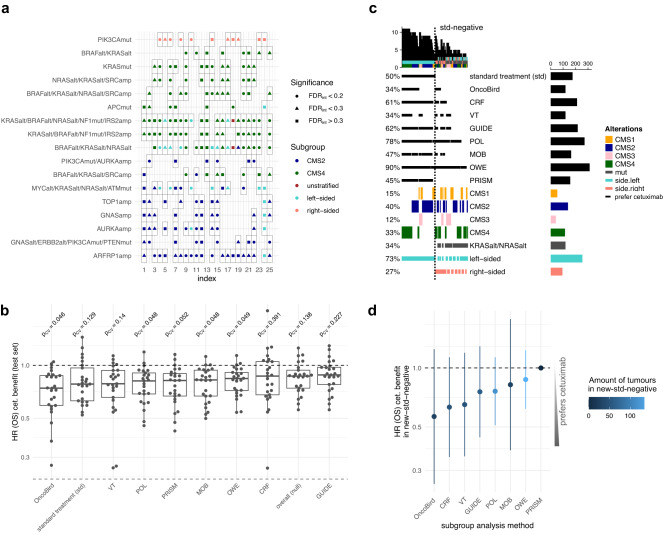
Precision medicine has revolutionised cancer treatments; however, actionable biomarkers remain scarce. To address this, we develop the Oncology Biomarker Discovery (OncoBird) framework for analysing the molecular and biomarker landscape of randomised controlled clinical trials. OncoBird identifies biomarkers based on single genes or mutually exclusive genetic alterations in isolation or in the context of tumour subtypes, and finally, assesses predictive components by their treatment interactions. Here, we utilise the open-label, randomised phase III trial (FIRE-3, AIO KRK-0306) in metastatic colorectal carcinoma patients, who received either cetuximab or bevacizumab in combination with 5-fluorouracil, folinic acid and irinotecan (FOLFIRI). We systematically identify five biomarkers with predictive components, e.g., patients with tumours that carry chr20q amplifications or lack mutually exclusive ERK signalling mutations benefited from cetuximab compared to bevacizumab. In summary, OncoBird characterises the molecular landscape and outlines actionable biomarkers, which generalises to any molecularly characterised randomised controlled trial.
© 2023. Springer Nature Limited.
Conflict of interest statement
A.S. served on advisory boards for BMS and Novocure, received honoraria for talks by Roche, Servier and Taiho Pharmaceuticals and received reimbursement for travel by Roche, Merck KGaA, MSD Sharp & Dohme, Pfizer, Lilly Oncology, and Amgen. V.H., S.S. and D.P.M. received honoraria for talks, advisory boards and travel expenses by Merck KGaA, Amgen, Roche, Pfizer, BMS, MSD, AstraZeneca, Novartis, Terumo, Oncosil, Nordic, Seagen, GSK, Takeda, Servier, Pierre Fabre, Taiho, Lilly Oncology, Servier, Sanofi and Bayer Pharmaceuticals. M.P.M. is a former employee at AstraZeneca, academically collaborates with AstraZeneca, GSK and Roche, and receives funding from GSK and Roche. J.W.H. served on an advisory board for Roche, has received honoraria from Roche, and travel support from Novartis. M.M. received honoraria for advisory boards or talks by Amgen, BMS, Roche, Merck KGaA, MSD Sharp & Dohme, Lilly Oncology, Servier, Pierre Fabre, Taiho Sanofi and Bayer Pharmaceuticals and serves as officer for the European Organisation on Research and Treatment of Cancer (EORTC), and Arbeitsgemeinschaft internistische Onkologie (AIO). C.B.W. has received honoraria from Amgen, Bayer, Chugai, Celgene, GSK, MSD, Merck, Janssen, Ipsen, Roche, Servier, SIRTeX, Taiho; served on advisory boards for Bayer, BMS, Celgene, Servier, Shire/Baxalta, Rafael Pharmaceuticals, RedHill, Roche, has received travel support by Bayer, Celgene, RedHill, Roche, Servier, Taiho and research grants (institutional) by Roche. C.B.W. serves as an officer for the European Society of Medical Oncology (ESMO), Deutsche Krebshilfe (DKH) and AIO. The remaining authors declare no competing interests.
Figures
Similar articles
-
FOLFIRI plus cetuximab or bevacizumab for advanced colorectal cancer: final survival and per-protocol analysis of FIRE-3, a randomised clinical trial.Br J Cancer. 2021 Feb;124(3):587-594. doi: 10.1038/s41416-020-01140-9. Epub 2020 Nov 6. Br J Cancer. 2021. PMID: 33154570 Free PMC article. Clinical Trial.
-
FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer (FIRE-3): a randomised, open-label, phase 3 trial.Lancet Oncol. 2014 Sep;15(10):1065-75. doi: 10.1016/S1470-2045(14)70330-4. Epub 2014 Jul 31. Lancet Oncol. 2014. PMID: 25088940 Clinical Trial.
-
Mutational profiles of metastatic colorectal cancer treated with FOLFIRI plus cetuximab or bevacizumab before and after secondary resection (AIO KRK 0306; FIRE-3).Int J Cancer. 2021 Dec 1;149(11):1935-1943. doi: 10.1002/ijc.33747. Epub 2021 Jul 31. Int J Cancer. 2021. PMID: 34310714
-
Systematic review and economic evaluation of bevacizumab and cetuximab for the treatment of metastatic colorectal cancer.Health Technol Assess. 2007 Mar;11(12):1-128, iii-iv. doi: 10.3310/hta11120. Health Technol Assess. 2007. PMID: 17346499 Review.
-
Integration of novel agents in the treatment of colorectal cancer.Cancer Chemother Pharmacol. 2004 Sep;54 Suppl 1:S32-9. doi: 10.1007/s00280-004-0884-0. Cancer Chemother Pharmacol. 2004. PMID: 15309512 Review.
Cited by
-
Unraveling temporal and spatial biomarkers of epithelial-mesenchymal transition in colorectal cancer: insights into the crucial role of immunosuppressive cells.J Transl Med. 2023 Nov 8;21(1):794. doi: 10.1186/s12967-023-04600-x. J Transl Med. 2023. PMID: 37940972 Free PMC article.
-
Toward Precision in Critical Care Research: Methods for Observational and Interventional Studies.Crit Care Med. 2024 Sep 1;52(9):1439-1450. doi: 10.1097/CCM.0000000000006371. Epub 2024 Aug 15. Crit Care Med. 2024. PMID: 39145702 Review.
-
Biomarker-Guided Tailored Therapy in Major Depression.Adv Exp Med Biol. 2024;1456:379-400. doi: 10.1007/978-981-97-4402-2_19. Adv Exp Med Biol. 2024. PMID: 39261439 Review.
-
Colitis-associated carcinogenesis: crosstalk between tumors, immune cells and gut microbiota.Cell Biosci. 2023 Oct 24;13(1):194. doi: 10.1186/s13578-023-01139-8. Cell Biosci. 2023. PMID: 37875976 Free PMC article. Review.
References
-
- Ting, N., Cappelleri, J. C., Ho, S. & Chen, D.-G. (eds) Design and Analysis of Subgroups with Biopharmaceutical Applications (Springer, 2020).
-
- European Medicines Agency. Guideline on the Investigation of Subgroups in Confirmatory Clinical Trials. Draft. European Medicines Agency/Committee for Medicinal Products for Human Use. EMA/CHMP/539146/2013 (EMA, 2014).
-
- Loh W, Cao L, Zhou P. Subgroup identification for precision medicine: a comparative review of 13 methods. Wiley Interdiscip. Rev. Data Min. Knowl. Discov. 2019;9:e1326. doi: 10.1002/widm.1326. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
