

Associations between eGFR and albuminuria with right ventricular measures: the MESA-Right Ventricle study
- PMID: 37664568
- PMCID: PMC10469092
- DOI: 10.1093/ckj/sfad096
Associations between eGFR and albuminuria with right ventricular measures: the MESA-Right Ventricle study
Abstract
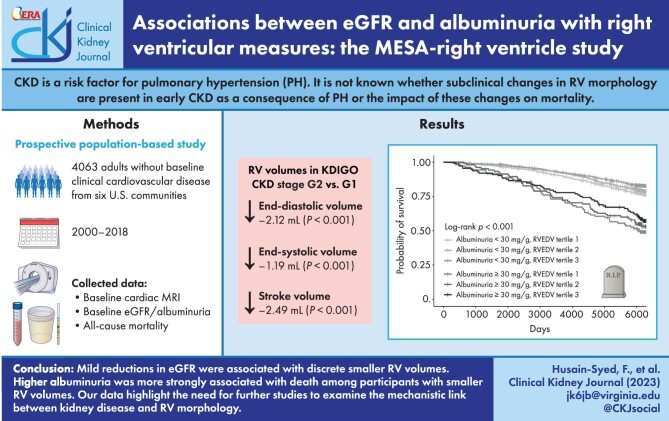
Background: Chronic kidney disease (CKD) is associated with an increased risk of pulmonary hypertension, which may lead to right ventricular (RV) pressure overload and RV dysfunction. However, the presence of subclinical changes in RV structure or function in early CKD and the influence of these changes on mortality are not well studied. We hypothesized that early CKD, as indicated by elevated albuminuria or mild reductions in estimated glomerular filtration rate (eGFR), is associated with greater RV dilation and RV mass.
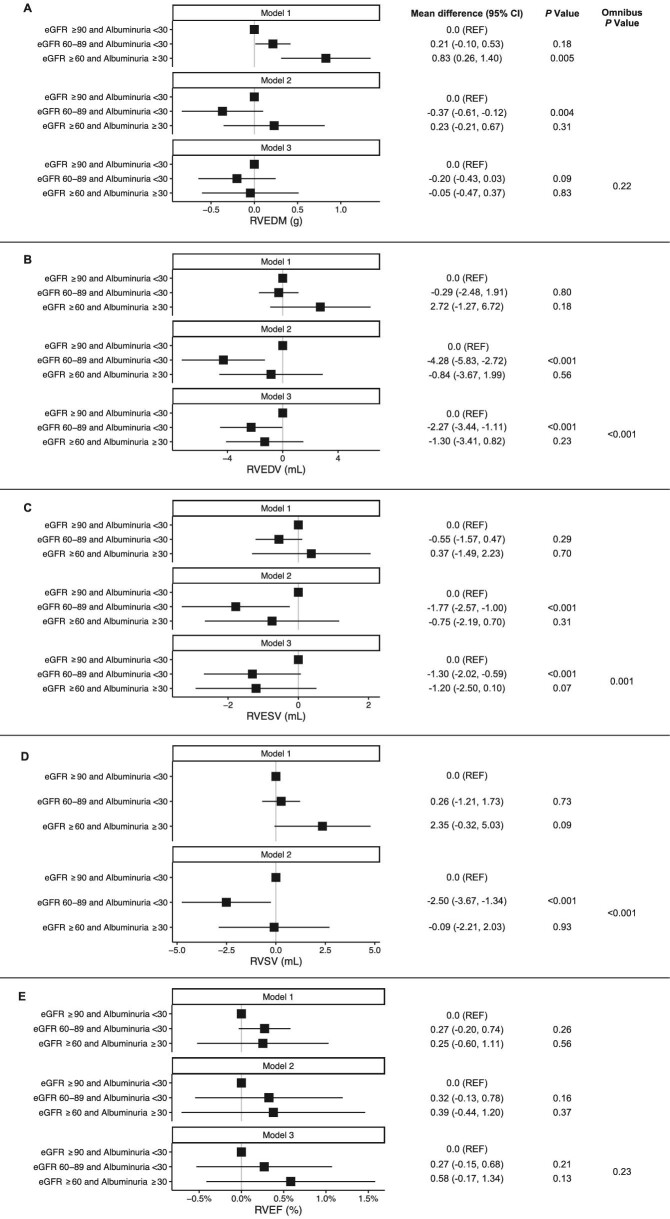
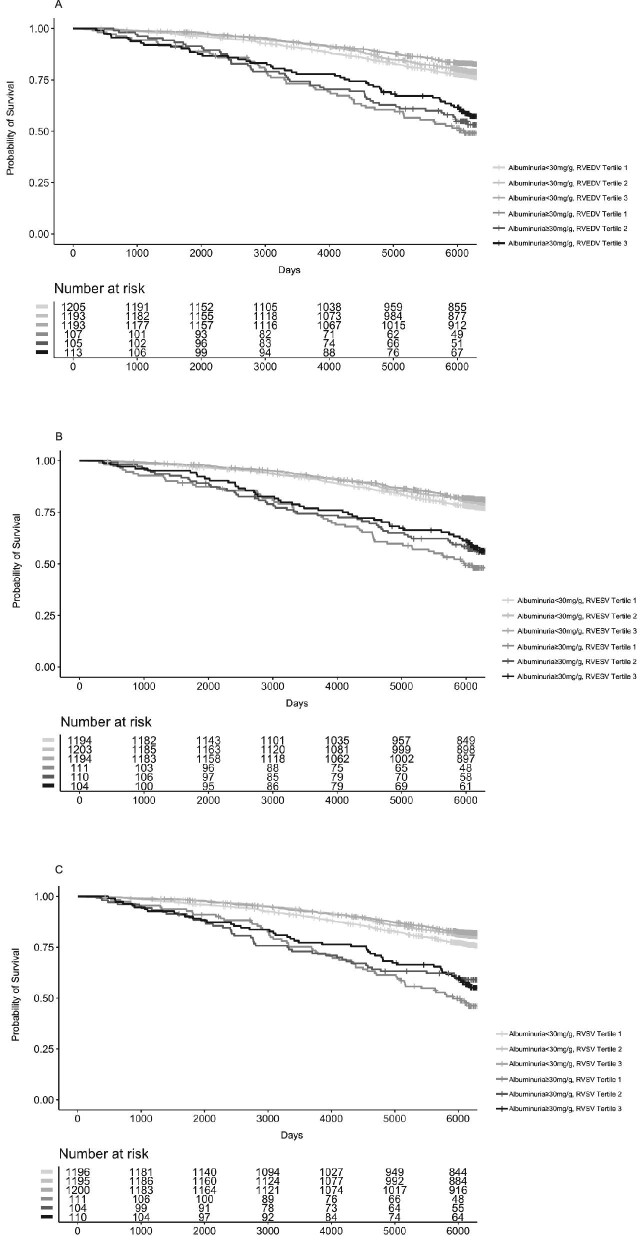
Methods: We included 4063 participants (age 45-84 years) without baseline clinical cardiovascular disease from the Multi-Ethnic Study of Atherosclerosis. The associations of baseline creatinine-cystatin C-based eGFR and albuminuria with cardiac magnetic resonance-derived RV measures (2000-02) were examined cross-sectionally with linear regression models. Cox regression models were used to examine whether RV parameters modified the associations of eGFR and albuminuria with all-cause mortality.
Results: Participants with reductions in eGFR primarily within the 60-89 mL/min/1.73 m2 category had smaller RV end-diastolic and end-systolic volumes and stroke volume (all adjusted P-trends <.001) than those with eGFR ≥90 mL/min/1.73 m2, an association that was predominantly seen in participants with albuminuria below 30 mg/g creatinine. Albuminuria was more strongly associated with death among those with lower RV volumes (P-values for interaction <.03).
Conclusions: Among community-dwelling adults, reductions in eGFR primarily within the normal range were associated with smaller RV volumes and the association of albuminuria with worse survival was stronger among those with smaller RV volumes. Further studies are needed to elucidate the underlying mechanistic pathways that link kidney measures and RV morphology.
Keywords: cardiac magnetic resonance; cardiorenal syndromes; chronic kidney disease; kidney function; pulmonary hypertension.
© The Author(s) 2023. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
J.S.K. receives grant support from the National Heart, Lung, and Blood Institute (NHLBI). All other authors have declared that no conflict of interests exists. The results presented in this paper have not been presented or published previously in whole or part nor in abstract form.
Figures
Similar articles
-
Low serum bicarbonate and kidney function decline: the Multi-Ethnic Study of Atherosclerosis (MESA).Am J Kidney Dis. 2014 Oct;64(4):534-41. doi: 10.1053/j.ajkd.2014.05.008. Epub 2014 Jun 18. Am J Kidney Dis. 2014. PMID: 24953891 Free PMC article.
-
Kidney Function as Risk Factor and Predictor of Cardiovascular Outcomes and Mortality Among Older Adults.Am J Kidney Dis. 2021 Mar;77(3):386-396.e1. doi: 10.1053/j.ajkd.2020.09.015. Epub 2020 Nov 14. Am J Kidney Dis. 2021. PMID: 33197533
-
Kidney Disease Measures and Left Ventricular Structure and Function: The Atherosclerosis Risk in Communities Study.J Am Heart Assoc. 2017 Sep 22;6(9):e006259. doi: 10.1161/JAHA.117.006259. J Am Heart Assoc. 2017. PMID: 28939714 Free PMC article.
-
Kidney Disease in Diabetes.In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 22. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 22. PMID: 33651560 Free Books & Documents. Review.
-
Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: a meta-analysis.Lancet. 2012 Nov 10;380(9854):1649-61. doi: 10.1016/S0140-6736(12)61272-0. Epub 2012 Sep 24. Lancet. 2012. PMID: 23013600 Free PMC article. Review.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
