

Recent advances in poor HIV immune reconstitution: what will the future look like?
- PMID: 37608956
- PMCID: PMC10440441
- DOI: 10.3389/fmicb.2023.1236460
Recent advances in poor HIV immune reconstitution: what will the future look like?
Abstract
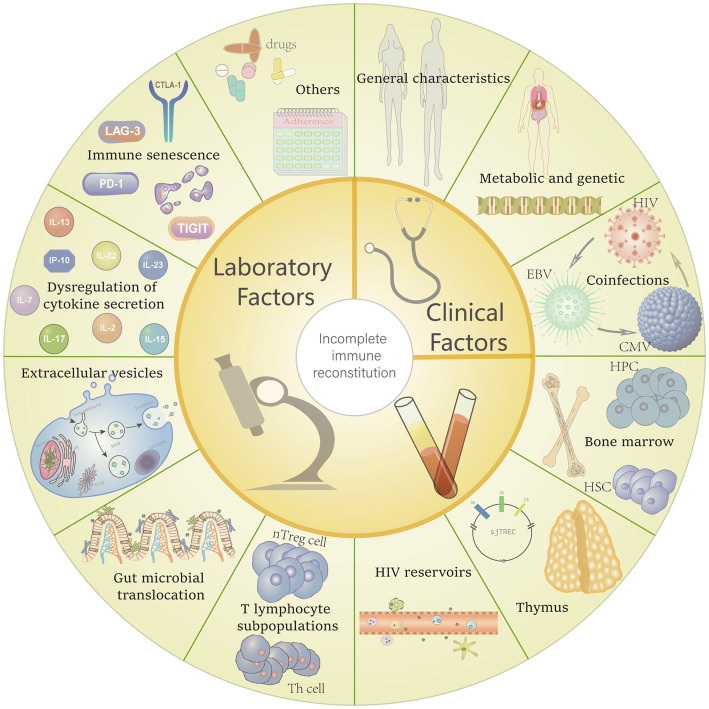
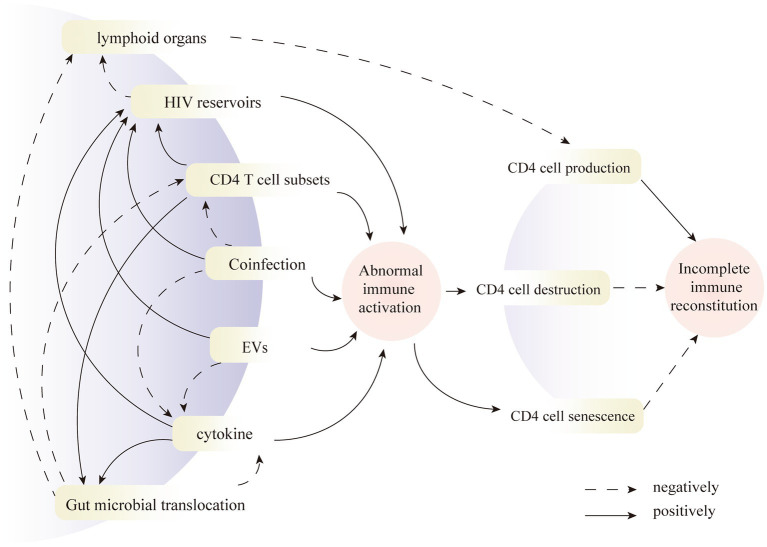
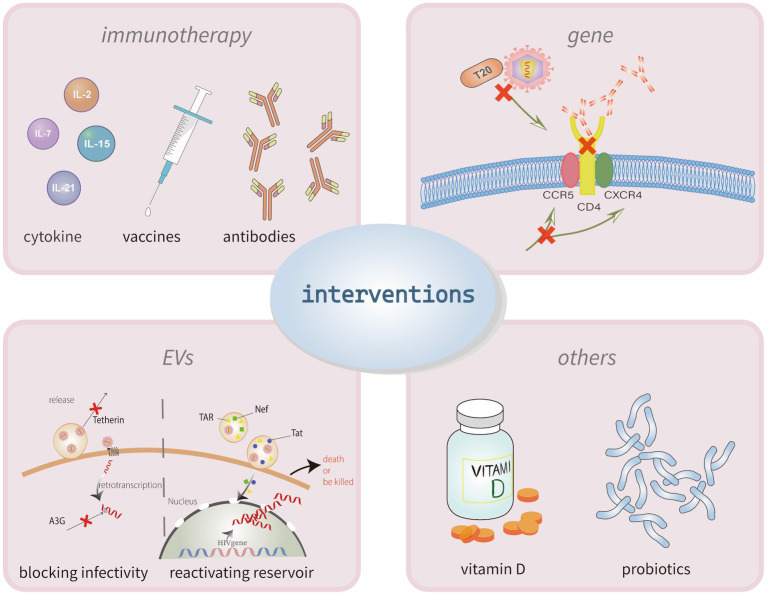
Combination antiretroviral therapy has demonstrated proved effectiveness in suppressing viral replication and significantly recovering CD4+ T cell count in HIV type-1 (HIV-1)-infected patients, contributing to a dramatic reduction in AIDS morbidity and mortality. However, the factors affecting immune reconstitution are extremely complex. Demographic factors, co-infection, baseline CD4 cell level, abnormal immune activation, and cytokine dysregulation may all affect immune reconstitution. According to report, 10-40% of HIV-1-infected patients fail to restore the normalization of CD4+ T cell count and function. They are referred to as immunological non-responders (INRs) who fail to achieve complete immune reconstitution and have a higher mortality rate and higher risk of developing other non-AIDS diseases compared with those who achieve complete immune reconstitution. Heretofore, the mechanisms underlying incomplete immune reconstitution in HIV remain elusive, and INRs are not effectively treated or mitigated. This review discusses the recent progress of mechanisms and factors responsible for incomplete immune reconstitution in AIDS and summarizes the corresponding therapeutic strategies according to different mechanisms to improve the individual therapy.
Keywords: CD4+ T cells; HIV-1 infection; immune reconstitution; immunological non-responders; therapeutic interventions.
Copyright © 2023 Zhang and Ruan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Incomplete immune reconstitution in HIV/AIDS patients on antiretroviral therapy: Challenges of immunological non-responders.J Leukoc Biol. 2020 Apr;107(4):597-612. doi: 10.1002/JLB.4MR1019-189R. Epub 2020 Jan 22. J Leukoc Biol. 2020. PMID: 31965635 Free PMC article. Review.
-
The predictive role of CD4+ cell count and CD4/CD8 ratio in immune reconstitution outcome among HIV/AIDS patients receiving antiretroviral therapy: an eight-year observation in China.BMC Immunol. 2019 Aug 28;20(1):31. doi: 10.1186/s12865-019-0311-2. BMC Immunol. 2019. PMID: 31455209 Free PMC article.
-
Failure of CD4+ T-cell Recovery upon Virally-Effective cART: an Enduring Gap in the Understanding of HIV+ Immunological non-Responders.New Microbiol. 2022 Jul;45(3):155-172. New Microbiol. 2022. PMID: 35920870 Review.
-
Decreased CD73+ Double-Negative T Cells and Elevated Level of Soluble CD73 Correlated With and Predicted Poor Immune Reconstitution in HIV-Infected Patients After Antiretroviral Therapy.Front Immunol. 2022 Apr 4;13:869286. doi: 10.3389/fimmu.2022.869286. eCollection 2022. Front Immunol. 2022. PMID: 35444646 Free PMC article.
-
Low Double-Negative CD3+CD4-CD8- T Cells Are Associated with Incomplete Restoration of CD4+ T Cells and Higher Immune Activation in HIV-1 Immunological Non-Responders.Front Immunol. 2016 Dec 9;7:579. doi: 10.3389/fimmu.2016.00579. eCollection 2016. Front Immunol. 2016. PMID: 28018346 Free PMC article.
Cited by
-
Investigating the Determinants of Mortality before CD4 Count Recovery in a Cohort of Patients Initiated on Antiretroviral Therapy in South Africa Using a Fine and Gray Competing Risks Model.Trop Med Infect Dis. 2024 Jul 10;9(7):154. doi: 10.3390/tropicalmed9070154. Trop Med Infect Dis. 2024. PMID: 39058196 Free PMC article.
-
Factors Associated with Neutralizing Antibody Responses following 2-Dose and 3rd Booster Monovalent COVID-19 Vaccination in Japanese People Living with HIV.Viruses. 2024 Apr 2;16(4):555. doi: 10.3390/v16040555. Viruses. 2024. PMID: 38675897 Free PMC article.
References
-
- Adolescents., P.O.A.G.F.A.A (2021). Guidelines for the use of antiretroviral agents in adults and adolescents with HIV. Department of Health and Human Services.
-
- Ahn M. Y., Jiamsakul A., Khusuwan S., Khol V., Pham T. T., Chaiwarith R., et al. . (2019). The influence of age-associated comorbidities on responses to combination antiretroviral therapy in older people living with HIV. J. Int. AIDS Soc. 22:e25228. doi: 10.1002/jia2.25228, PMID: - DOI - PMC - PubMed
-
- Arenaccio C., Chiozzini C., Columba-Cabezas S., Manfredi F., Affabris E., Baur A., et al. . (2014). Exosomes from human immunodeficiency virus type 1 (HIV-1)-infected cells license quiescent CD4+ T lymphocytes to replicate HIV-1 through a Nef- and ADAM17-dependent mechanism. J. Virol. 88, 11529–11539. doi: 10.1128/JVI.01712-14, PMID: - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials