

Interleukin-6 in Patients With Heart Failure and Preserved Ejection Fraction
- PMID: 37565977
- PMCID: PMC10895473
- DOI: 10.1016/j.jchf.2023.06.031
Interleukin-6 in Patients With Heart Failure and Preserved Ejection Fraction
Abstract
Background: Interleukin (IL)-6 is a central inflammatory mediator and potential therapeutic target in heart failure (HF). Prior studies have shown that IL-6 concentrations are elevated in patients with HF, but much fewer data are available in heart failure with preserved ejection fraction (HFpEF).
Objectives: This study aims to determine how IL-6 relates to changes in cardiac function, congestion, body composition, and exercise tolerance in HFpEF.
Methods: Clinical, laboratory, body composition, exercise capacity, physiologic and health status data across 4 National Heart, Lung, and Blood Institute-sponsored trials were analyzed according to the tertiles of IL-6.
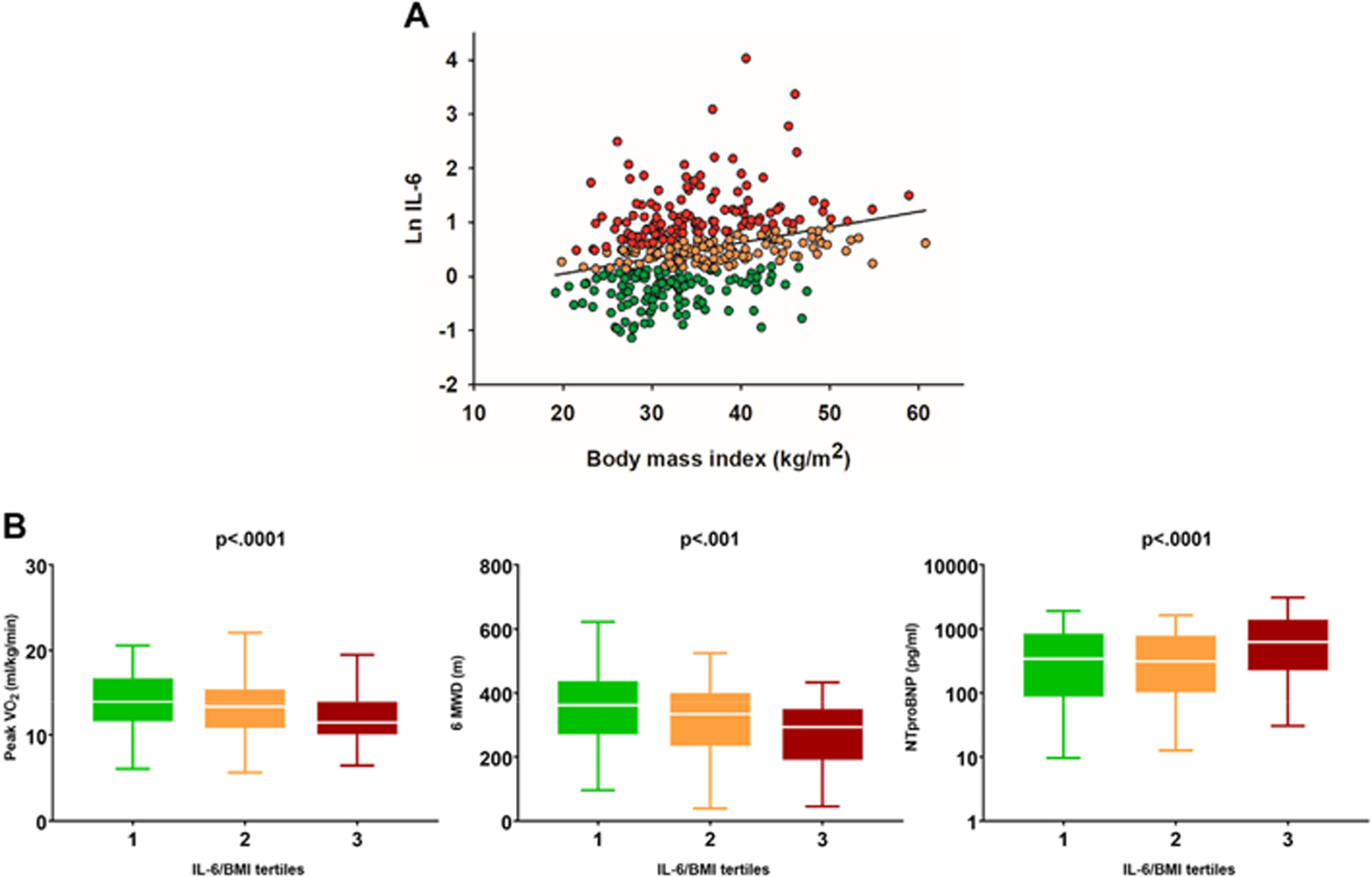
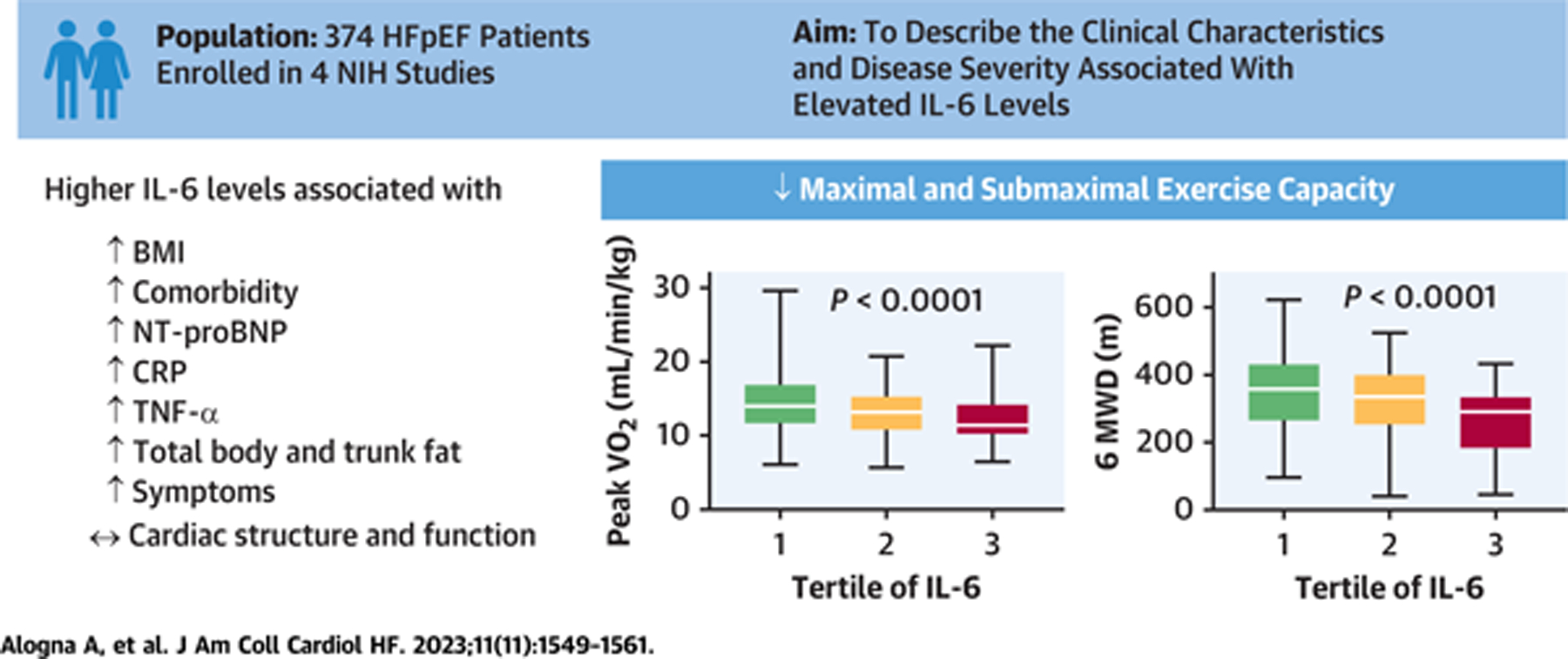
Results: IL-6 was measured in 374 patients with HFpEF. Patients with highest IL-6 levels had greater body mass index; higher N-terminal pro-B-type natriuretic peptide, C-reactive protein, and tumor necrosis factor-α levels; worse renal function; and lower hemoglobin levels, and were more likely to have diabetes. Although cardiac structure and function measured at rest were similar, patients with HFpEF and highest IL-6 concentrations had more severely impaired peak oxygen consumption (12.3 ± 3.3 mL/kg/min 13.1 ± 3.1 mL/kg/min 14.4 ± 3.9 mL/kg/min, P < 0.0001) as well as 6-minute walk distance (276 ± 107 m vs 332 ± 106 m vs 352 ± 116 m, P < 0.0001), even after accounting for increases in IL-6 related to excess body mass. IL-6 concentrations were associated with increases in total body fat and trunk fat, more severe symptoms during submaximal exercise, and poorer patient-reported health status.
Conclusions: IL-6 levels are commonly elevated in HFpEF, and are associated with greater symptom severity, poorer exercise capacity, and more upper body fat accumulation. These findings support testing the hypothesis that therapies that inhibit IL-6 in patients with HFpEF may improve clinical status. (Clinical Trial Registrations: Phosphodiesterase-5 Inhibition to Improve Clinical Status and Exercise Capacity in Diastolic Heart Failure [RELAX], NCT00763867; Nitrate's Effect on Activity Tolerance in Heart Failure With Preserved Ejection Fraction, NCT02053493; Inorganic Nitrite Delivery to Improve Exercise Capacity in HFpEF, NCT02742129; Inorganic Nitrite to Enhance Benefits From Exercise Training in Heart Failure With Preserved Ejection Fraction [HFpEF], NCT02713126).
Keywords: fat mass; heart failure with preserved ejection fraction; inflammation; interleukin-6; obesity.
Copyright © 2023 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures Dr Borlaug is supported by R01 HL128526, U01 HL160226, and R01 HL162828, from the National Institutes of Health (NIH), and W81XWH2210245, from the U.S. Department of Defense. Dr Alogna is supported by the Deutsche Forschungsgemeinschaft (DFG; CRC 1470, Z01). Drs Kirkland and Tchkonia are supported by R37 AG013925, P01 AG062413, and R33 AG061456 from NIH, the Connor Fund, Robert J. and Theresa W. Ryan, and the Noaber Foundation. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



Comment in
-
Paving the Road for Interleukin-6 Inhibition in Heart Failure With Preserved Ejection Fraction.JACC Heart Fail. 2023 Nov;11(11):1562-1564. doi: 10.1016/j.jchf.2023.06.032. Epub 2023 Aug 16. JACC Heart Fail. 2023. PMID: 37589616 No abstract available.
Similar articles
-
Quality of life in heart failure with preserved ejection fraction: importance of obesity, functional capacity, and physical inactivity.Eur J Heart Fail. 2020 Jun;22(6):1009-1018. doi: 10.1002/ejhf.1788. Epub 2020 Mar 9. Eur J Heart Fail. 2020. PMID: 32150314
-
Distinct Impact of Noncardiac Comorbidities on Exercise Capacity and Functional Status in Chronic Heart Failure.JACC Heart Fail. 2023 Oct;11(10):1365-1376. doi: 10.1016/j.jchf.2023.05.018. Epub 2023 Jun 28. JACC Heart Fail. 2023. PMID: 37389503
-
Characterization of the Obese Phenotype of Heart Failure With Preserved Ejection Fraction: A RELAX Trial Ancillary Study.Mayo Clin Proc. 2019 Jul;94(7):1199-1209. doi: 10.1016/j.mayocp.2018.11.037. Mayo Clin Proc. 2019. PMID: 31272568
-
INDIE-HFpEF (Inorganic Nitrite Delivery to Improve Exercise Capacity in Heart Failure With Preserved Ejection Fraction): Rationale and Design.Circ Heart Fail. 2017 May;10(5):e003862. doi: 10.1161/CIRCHEARTFAILURE.117.003862. Circ Heart Fail. 2017. PMID: 28476756 Free PMC article. Review.
-
The Effect of Weight Loss Through Lifestyle Interventions in Patients With Heart Failure With Preserved Ejection Fraction-A Systematic Review and Meta-Analysis of Randomised Controlled Trials.Heart Lung Circ. 2024 Feb;33(2):197-208. doi: 10.1016/j.hlc.2023.11.022. Epub 2024 Feb 6. Heart Lung Circ. 2024. PMID: 38320881 Review.
Cited by
-
A Set of Possible Markers for Monitoring Heart Failure and Cognitive Impairment Associated: A Review of Literature from the Past 5 Years.Biomolecules. 2024 Feb 3;14(2):185. doi: 10.3390/biom14020185. Biomolecules. 2024. PMID: 38397422 Free PMC article. Review.
-
Precision Phenotyping of Heart Failure in People with HIV: Early Insights and Challenges.Curr Heart Fail Rep. 2024 Aug;21(4):417-427. doi: 10.1007/s11897-024-00674-w. Epub 2024 Jun 28. Curr Heart Fail Rep. 2024. PMID: 38940893 Review.
-
Nutritional Support Reduces Circulating Cytokines in Patients with Heart Failure.Nutrients. 2024 May 27;16(11):1637. doi: 10.3390/nu16111637. Nutrients. 2024. PMID: 38892570 Free PMC article. Clinical Trial.
-
Effects of tirzepatide on circulatory overload and end-organ damage in heart failure with preserved ejection fraction and obesity: a secondary analysis of the SUMMIT trial.Nat Med. 2024 Nov 17. doi: 10.1038/s41591-024-03374-z. Online ahead of print. Nat Med. 2024. PMID: 39551891
-
Heart failure with preserved ejection fraction: implications for anaesthesia.BJA Educ. 2024 May;24(5):155-163. doi: 10.1016/j.bjae.2024.02.003. Epub 2024 Mar 6. BJA Educ. 2024. PMID: 38646450 Review. No abstract available.
References
-
- Murphy SP, Kakkar R, McCarthy CP, Januzzi JL Jr. Inflammation in heart failure: JACC State-of-the-Art Review. J Am Coll Cardiol 2020;75:1324–1340. - PubMed
-
- Adamo L, Rocha-Resende C, Prabhu SD, Mann DL. Reappraising the role of inflammation in heart failure. Nat Rev Cardiol 2020;17:269–285. - PubMed
-
- Paulus WJ, Tschope C. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol 2013;62:263–271. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
