

Effectiveness of Carbon Localization for Invasive Breast Cancer: An Institutional Experience
- PMID: 37496746
- PMCID: PMC10368511
- DOI: 10.1155/2023/4082501
Effectiveness of Carbon Localization for Invasive Breast Cancer: An Institutional Experience
Abstract
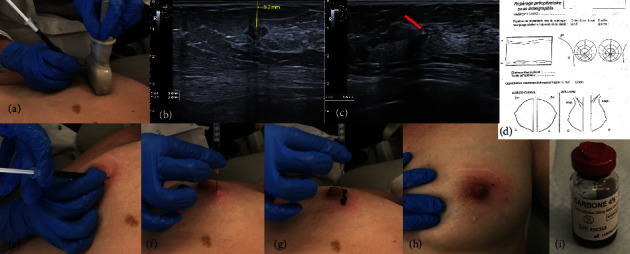
Introduction: The final oncological and aesthetic results of breast-conserving surgery (BCS) are influenced by the precise localization of breast cancer (BC) tumors and by the quality of the intraoperative margin assessment technique. This study aimed to assess the effectiveness of the carbon localization (CL) technique by determining the success rate of BC identification and the proportion of adequate complete resection of BC lesions.
Methods: We conducted a cross-sectional retrospective study of patients treated with primary BCS for invasive BC who underwent CL of their BC lesion at the Jules Bordet Institute between January 2015 and December 2017. Descriptive statistics with categorical and continuous variables were used. The success rate of tumor identification and the rate of adequate excision were calculated using the test of percentages for independent dichotomous data.
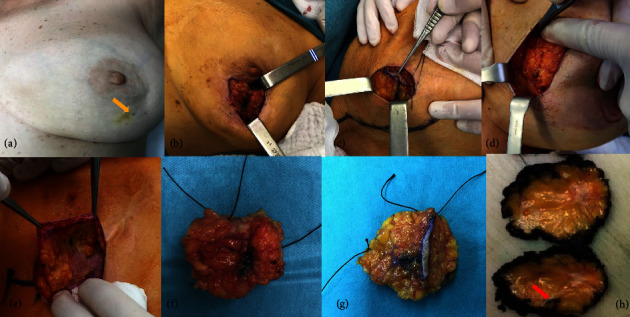
Results: This study included 542 patients with 564 nonpalpable BC lesions. The median pathological tumor size was 12 mm. Of these, 460 were invasive ductal carcinomas. Most of the tumors were of the luminal subtype. CL was performed using ultrasound guidance in 98.5% of cases. The median delay between CL and surgery was 5 days, with 46% of the patients having CL one day before surgery. The lumpectomy weighed 38 g on average, with a median diameter of the surgical sample at 6 cm and a median volume of 44 cm3 (6-369). One-stage complete resection was successfully performed in 93.4% of cases. In 36% of cases, an intraoperative re-excision was performed, based on intraoperative macroscopic pathological margin evaluation. The tumor was identified in 98.9% of cases in the breast surgical specimen.
Conclusion: This study demonstrated high success rates for BC tumor identification (99%) and one-stage complete resection (93.4%) after BCS and CL. These results show that CL is an effective, simple, and inexpensive localization technique for successful excision of BC lesions during BCS.
Copyright © 2023 Etienne El-Helou et al.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
Similar articles
-
Low re-excision rate for positive margins in patients treated with ultrasound-guided breast-conserving surgery.Breast. 2013 Oct;22(5):698-702. doi: 10.1016/j.breast.2012.12.019. Epub 2013 Jan 17. Breast. 2013. PMID: 23333255
-
Bracketed Localization in Breast-Conserving Surgery: Indications and Success Rates From a Single, High Volume, Academic Breast Cancer Center.Am Surg. 2023 Nov;89(11):4373-4378. doi: 10.1177/00031348221111516. Epub 2022 Jun 27. Am Surg. 2023. PMID: 35758520
-
Surgeon Variability and Factors Predicting for Reoperation Following Breast-Conserving Surgery.Ann Surg Oncol. 2018 Sep;25(9):2573-2578. doi: 10.1245/s10434-018-6526-2. Epub 2018 May 21. Ann Surg Oncol. 2018. PMID: 29786129 Free PMC article.
-
Surgeon performed continuous intraoperative ultrasound guidance decreases re-excisions and mastectomy rates in breast cancer.Breast. 2017 Jun;33:23-28. doi: 10.1016/j.breast.2017.02.014. Epub 2017 Mar 2. Breast. 2017. PMID: 28273552
-
Short term safety of oncoplastic breast conserving surgery for larger tumors.Eur J Surg Oncol. 2017 Apr;43(4):665-671. doi: 10.1016/j.ejso.2016.11.021. Epub 2016 Dec 18. Eur J Surg Oncol. 2017. PMID: 28041648
Cited by
-
Breast and axillary marking in the neoadjuvant setting: survey results from experts of the Brazilian society of mastology.Front Oncol. 2024 Oct 9;14:1393417. doi: 10.3389/fonc.2024.1393417. eCollection 2024. Front Oncol. 2024. PMID: 39445065 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
