

Rational use of inhaled corticosteroids for the treatment of COPD
- PMID: 37488104
- PMCID: PMC10366209
- DOI: 10.1038/s41533-023-00347-6
Rational use of inhaled corticosteroids for the treatment of COPD
Abstract
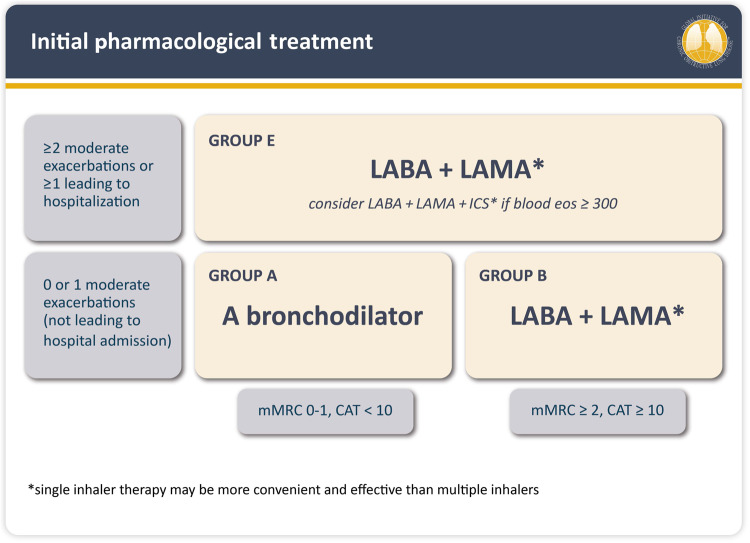
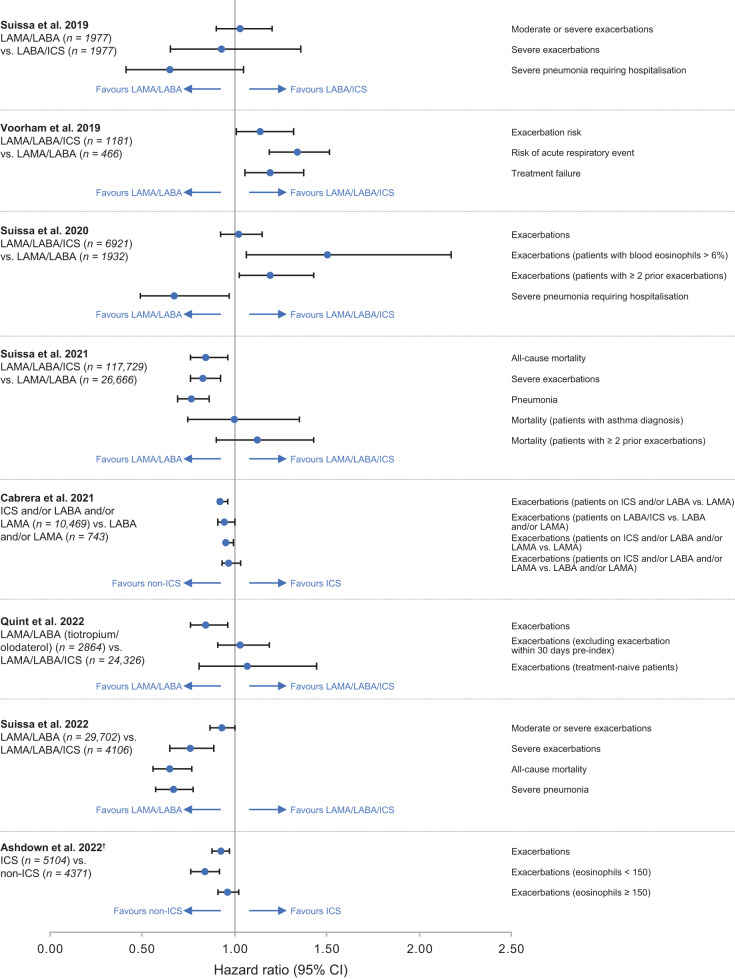
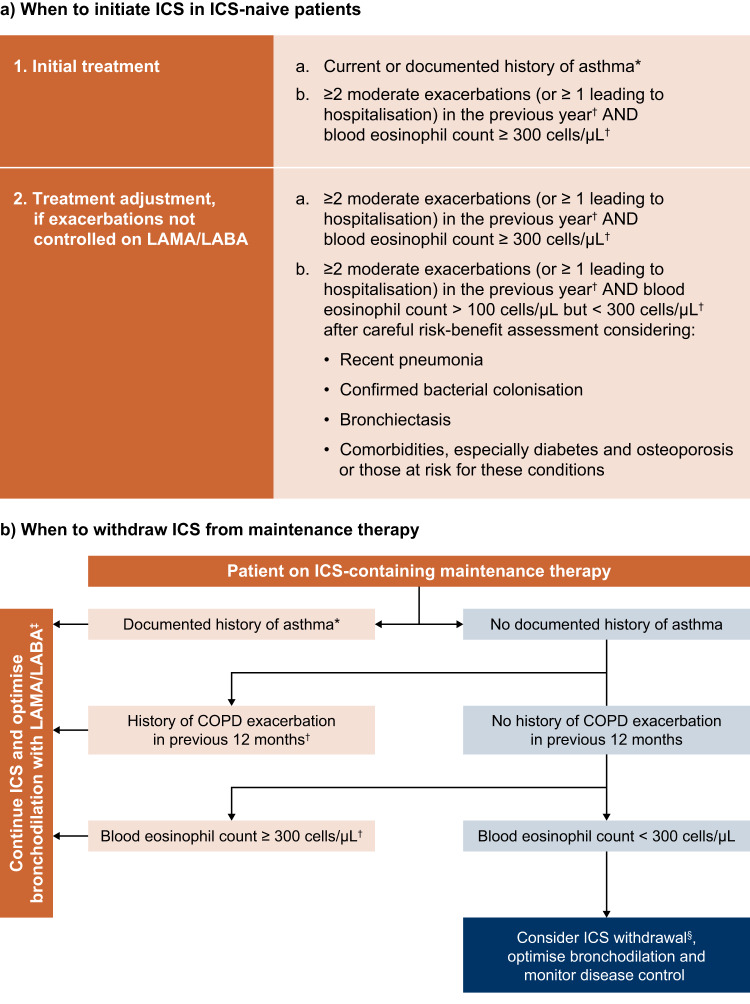
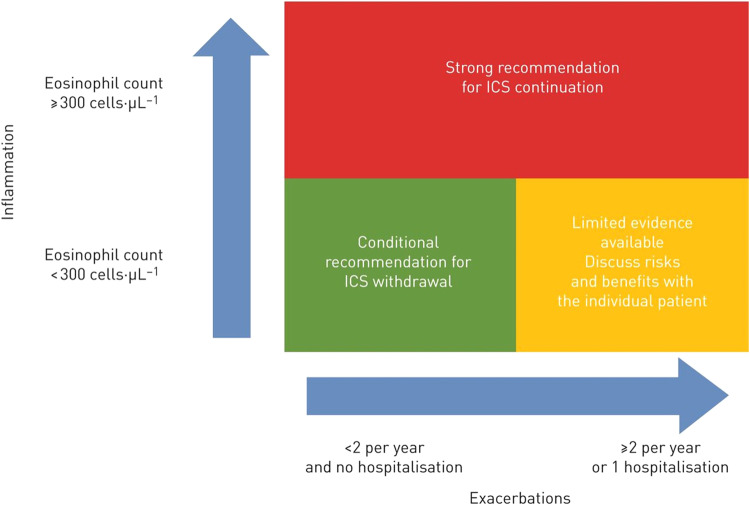
Inhaled corticosteroids (ICS) are the mainstay of treatment for asthma, but their role in chronic obstructive pulmonary disease (COPD) is debated. Recent randomised controlled trials (RCTs) conducted in patients with COPD and frequent or severe exacerbations demonstrated a significant reduction (~25%) in exacerbations with ICS in combination with dual bronchodilator therapy (triple therapy). However, the suggestion of a mortality benefit associated with ICS in these trials has since been rejected by the European Medicines Agency and US Food and Drug Administration. Observational evidence from routine clinical practice demonstrates that dual bronchodilation is associated with better clinical outcomes than triple therapy in a broad population of patients with COPD and infrequent exacerbations. This reinforces guideline recommendations that ICS-containing maintenance therapy should be reserved for patients with frequent or severe exacerbations and high blood eosinophils (~10% of the COPD population), or those with concomitant asthma. However, data from routine clinical practice indicate ICS overuse, with up to 50-80% of patients prescribed ICS. Prescription of ICS in patients not fulfilling guideline criteria puts patients at unnecessary risk of pneumonia and other long-term adverse events and also has cost implications, without any clear benefit in disease control. In this article, we review the benefits and risks of ICS use in COPD, drawing on evidence from RCTs and observational studies conducted in primary care. We also provide a practical guide to prescribing ICS, based on the latest global treatment guidelines, to help primary care providers identify patients for whom the benefits of ICS outweigh the risks.
© 2023. The Author(s).
Conflict of interest statement
J.K.Q. declares personal fees for advisory board participation or speaking fees from GlaxoSmithKline, Boehringer Ingelheim, AstraZeneca and Chiesi, but declares no non-financial competing interests. A.A. declares personal fees from AstraZeneca, and personal fees and non-financial support from Boehringer Ingelheim, outside the submitted work. P.J.B. declares research funding from AstraZeneca and Boehringer Ingelheim; consulting fees from AstraZeneca, Boehringer Ingelheim and Teva; and payment or honoraria for lectures, presentations, speaker bureaus, manuscript writing or educational events from AstraZeneca, Boehringer Ingelheim, Novartis and Teva. P.J.B. declares no non-financial competing interests.
Figures
Similar articles
-
Inhaled Corticosteroids for Chronic Obstructive Pulmonary Disease--The Shifting Treatment Paradigm.COPD. 2015;12(5):582-90. doi: 10.3109/15412555.2014.995288. Epub 2015 Mar 16. COPD. 2015. PMID: 25774769 Free PMC article. Review.
-
Assessing the healthcare resource use associated with inappropriate prescribing of inhaled corticosteroids for people with chronic obstructive pulmonary disease (COPD) in GOLD groups A or B: an observational study using the Clinical Practice Research Datalink (CPRD).Respir Res. 2018 Apr 11;19(1):63. doi: 10.1186/s12931-018-0767-2. Respir Res. 2018. PMID: 29642882 Free PMC article.
-
Inhaled corticosteroids versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2011 Dec 7;2011(12):CD007033. doi: 10.1002/14651858.CD007033.pub3. Cochrane Database Syst Rev. 2011. PMID: 22161409 Free PMC article. Review.
-
Inhaled corticosteroids versus long-acting beta(2)-agonists for chronic obstructive pulmonary disease.Cochrane Database Syst Rev. 2011 Oct 5;(10):CD007033. doi: 10.1002/14651858.CD007033.pub2. Cochrane Database Syst Rev. 2011. Update in: Cochrane Database Syst Rev. 2011 Dec 07;(12):CD007033. doi: 10.1002/14651858.CD007033.pub3 PMID: 21975759 Updated. Review.
-
Blood Eosinophil Counts, Withdrawal of Inhaled Corticosteroids and Risk of COPD Exacerbations and Mortality in the Clinical Practice Research Datalink (CPRD).COPD. 2019 Apr;16(2):152-159. doi: 10.1080/15412555.2019.1608172. Epub 2019 May 23. COPD. 2019. PMID: 31117850
Cited by
-
National Development in the Use of Inhaled Corticosteroid Treatment in Chronic Obstructive Pulmonary Disease: Repeated Cross-Sectional Studies from 1998 to 2018.Biomedicines. 2024 Feb 5;12(2):372. doi: 10.3390/biomedicines12020372. Biomedicines. 2024. PMID: 38397973 Free PMC article.
-
The Current Molecular and Cellular Landscape of Chronic Obstructive Pulmonary Disease (COPD): A Review of Therapies and Efforts towards Personalized Treatment.Proteomes. 2024 Aug 16;12(3):23. doi: 10.3390/proteomes12030023. Proteomes. 2024. PMID: 39189263 Free PMC article. Review.
-
Eligibility of patients with chronic obstructive pulmonary disease for inclusion in randomised control trials investigating triple therapy: a study using routinely collected data.Respir Res. 2024 Jan 18;25(1):43. doi: 10.1186/s12931-024-02672-x. Respir Res. 2024. PMID: 38238769 Free PMC article.
-
Intraclass comparison of inhaled corticosteroids for the risk of pneumonia in chronic obstructive pulmonary airway disorder: a network meta-analysis and meta-regression.Int J Clin Pharm. 2024 Aug;46(4):831-842. doi: 10.1007/s11096-024-01736-8. Epub 2024 Apr 25. Int J Clin Pharm. 2024. PMID: 38664319 Review.
-
Inhaled corticosteroid treatment and pneumonia in patients with chronic obstructive pulmonary disease - nationwide development from 1998 to 2018.Eur Clin Respir J. 2024 May 29;11(1):2359768. doi: 10.1080/20018525.2024.2359768. eCollection 2024. Eur Clin Respir J. 2024. PMID: 38817947 Free PMC article.
References
-
- Global Initiative for Asthma. Global strategy for asthma management and prevention, https://ginasthma.org/wp-content/uploads/2022/05/GINA-Main-Report-2022-F... (2022).
-
- Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: 2023 report. https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2... (2022).
