

Diabetic Foot Ulcers: A Review
- PMID: 37395769
- PMCID: PMC10723802
- DOI: 10.1001/jama.2023.10578
Diabetic Foot Ulcers: A Review
Abstract
Importance: Approximately 18.6 million people worldwide are affected by a diabetic foot ulcer each year, including 1.6 million people in the United States. These ulcers precede 80% of lower extremity amputations among people diagnosed with diabetes and are associated with an increased risk of death.
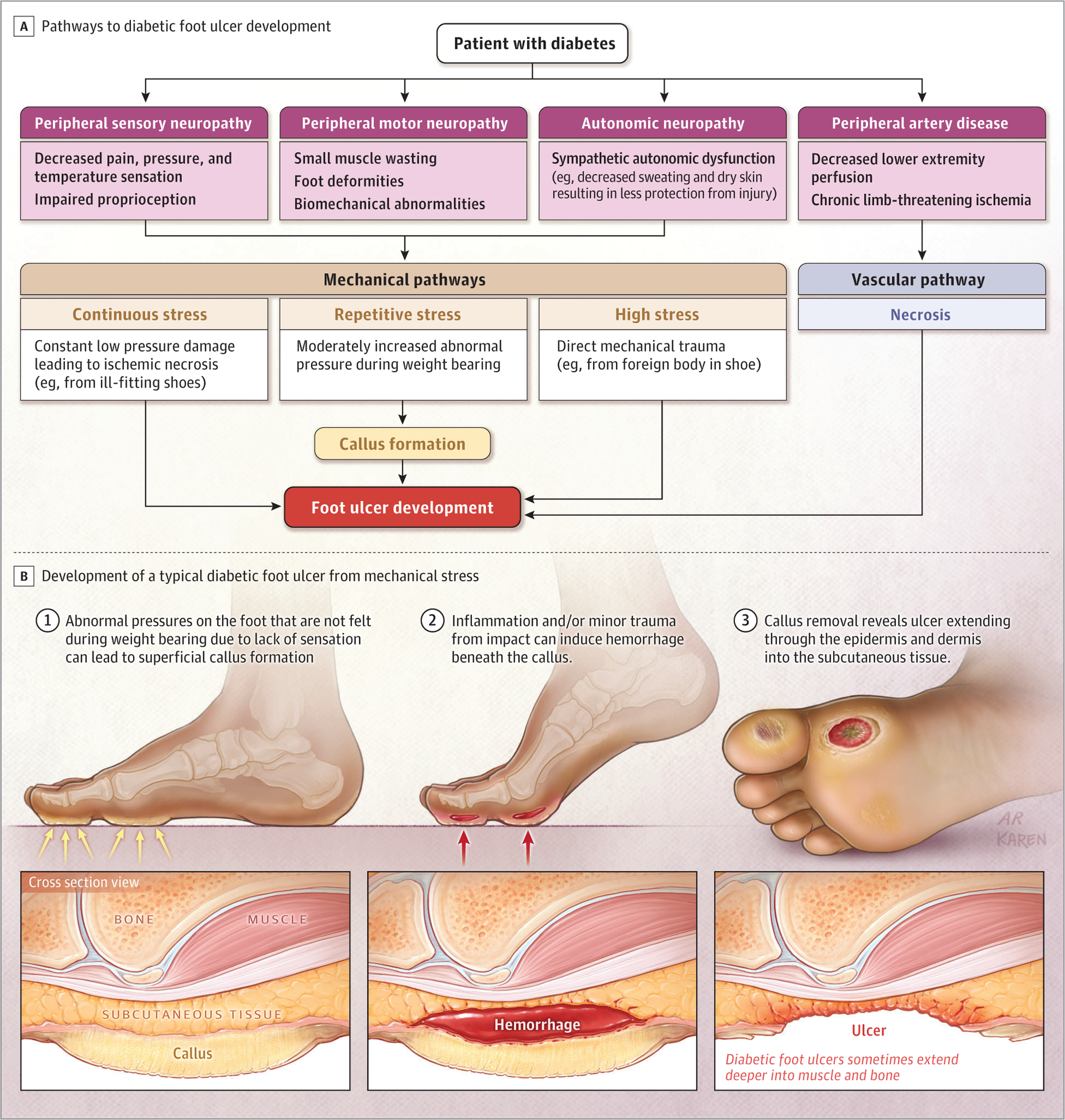
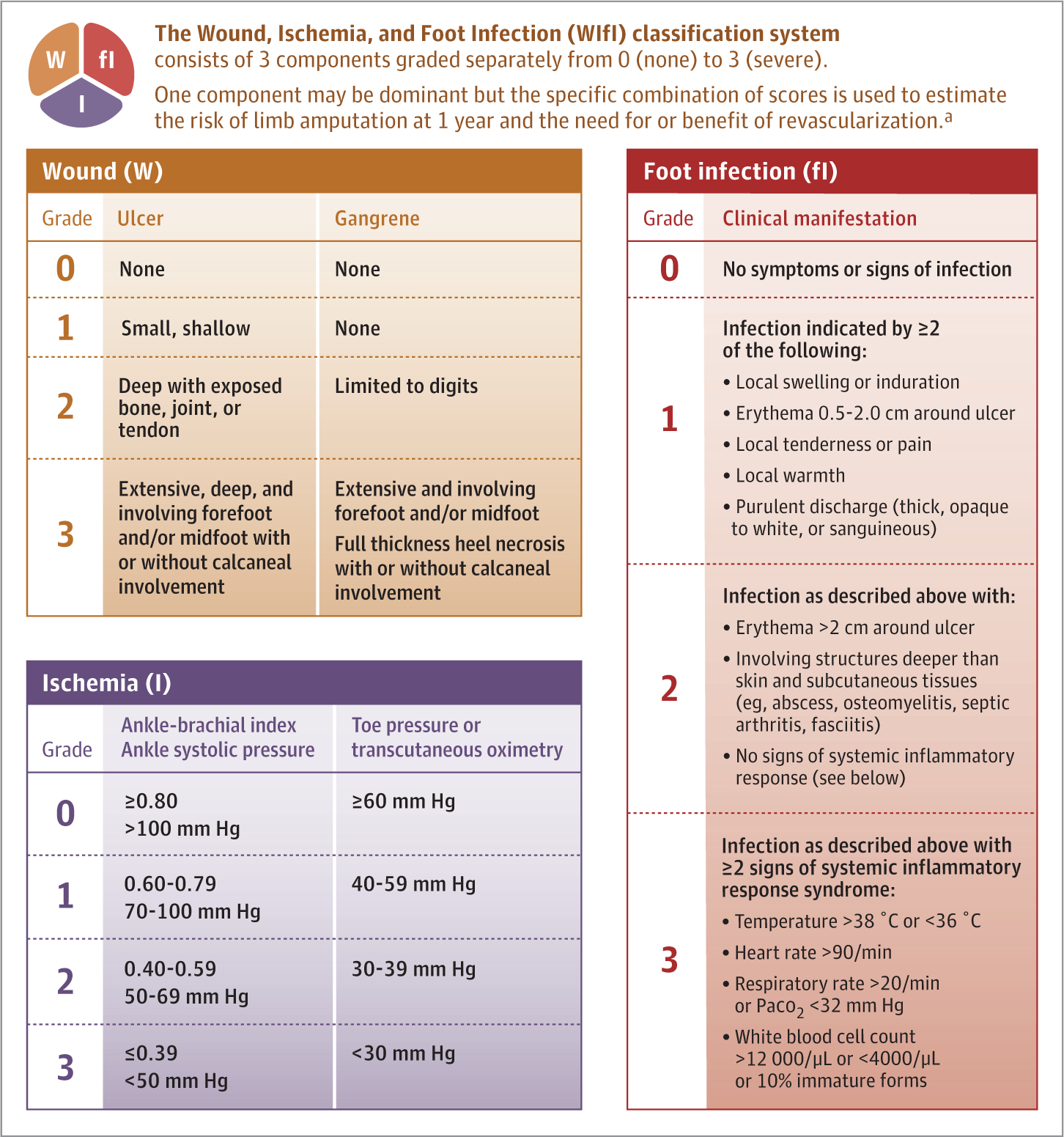
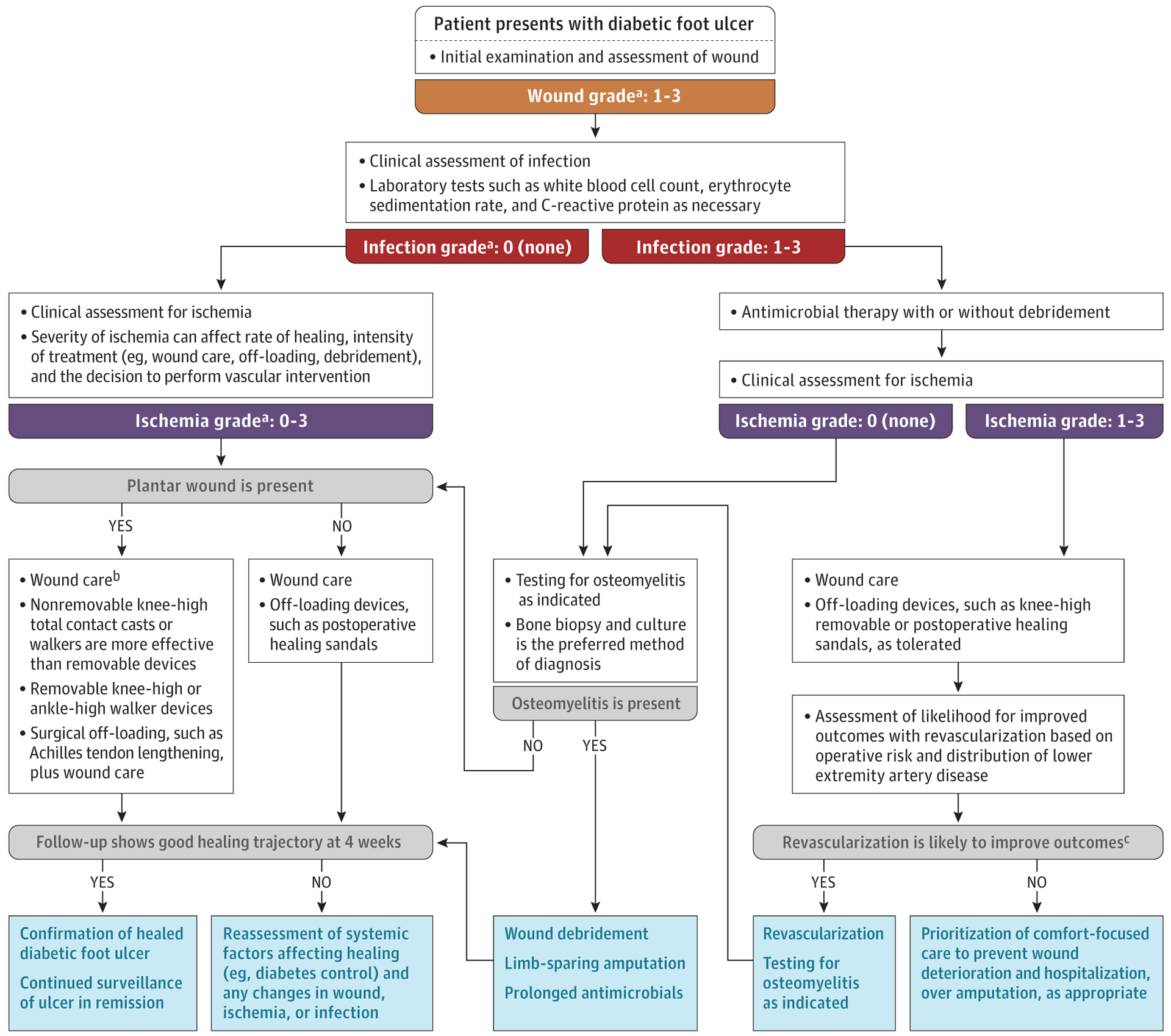
Observations: Neurological, vascular, and biomechanical factors contribute to diabetic foot ulceration. Approximately 50% to 60% of ulcers become infected, and about 20% of moderate to severe infections lead to lower extremity amputations. The 5-year mortality rate for individuals with a diabetic foot ulcer is approximately 30%, exceeding 70% for those with a major amputation. The mortality rate for people with diabetic foot ulcers is 231 deaths per 1000 person-years, compared with 182 deaths per 1000 person-years in people with diabetes without foot ulcers. People who are Black, Hispanic, or Native American and people with low socioeconomic status have higher rates of diabetic foot ulcer and subsequent amputation compared with White people. Classifying ulcers based on the degree of tissue loss, ischemia, and infection can help identify risk of limb-threatening disease. Several interventions reduce risk of ulcers compared with usual care, such as pressure-relieving footwear (13.3% vs 25.4%; relative risk, 0.49; 95% CI, 0.28-0.84), foot skin measurements with off-loading when hot spots (ie, greater than 2 °C difference between the affected foot and the unaffected foot) are found (18.7% vs 30.8%; relative risk, 0.51; 95% CI, 0.31-0.84), and treatment of preulcer signs. Surgical debridement, reducing pressure from weight bearing on the ulcer, and treating lower extremity ischemia and foot infection are first-line therapies for diabetic foot ulcers. Randomized clinical trials support treatments to accelerate wound healing and culture-directed oral antibiotics for localized osteomyelitis. Multidisciplinary care, typically consisting of podiatrists, infectious disease specialists, and vascular surgeons, in close collaboration with primary care clinicians, is associated with lower major amputation rates relative to usual care (3.2% vs 4.4%; odds ratio, 0.40; 95% CI, 0.32-0.51). Approximately 30% to 40% of diabetic foot ulcers heal at 12 weeks, and recurrence after healing is estimated to be 42% at 1 year and 65% at 5 years.
Conclusions and relevance: Diabetic foot ulcers affect approximately 18.6 million people worldwide each year and are associated with increased rates of amputation and death. Surgical debridement, reducing pressure from weight bearing, treating lower extremity ischemia and foot infection, and early referral for multidisciplinary care are first-line therapies for diabetic foot ulcers.
Conflict of interest statement
Figures
Comment in
-
Review of Diabetic Foot Ulcers.JAMA. 2023 Nov 7;330(17):1694-1695. doi: 10.1001/jama.2023.17197. JAMA. 2023. PMID: 37934224 No abstract available.
-
Review of Diabetic Foot Ulcers.JAMA. 2023 Nov 7;330(17):1695. doi: 10.1001/jama.2023.17191. JAMA. 2023. PMID: 37934225 No abstract available.
Similar articles
-
Treatment of diabetic foot ulcers.J Cardiovasc Surg (Torino). 2009 Jun;50(3):275-91. J Cardiovasc Surg (Torino). 2009. PMID: 19543189 Review.
-
Topical antimicrobial agents for treating foot ulcers in people with diabetes.Cochrane Database Syst Rev. 2017 Jun 14;6(6):CD011038. doi: 10.1002/14651858.CD011038.pub2. Cochrane Database Syst Rev. 2017. PMID: 28613416 Free PMC article. Review.
-
Poorly designed research does not help clarify the role of hyperbaric oxygen in the treatment of chronic diabetic foot ulcers.Diving Hyperb Med. 2016 Sep;46(3):133-134. Diving Hyperb Med. 2016. PMID: 27723012
-
[Prevention of diabetic foot].Acta Med Croatica. 2013 Oct;67 Suppl 1:35-44. Acta Med Croatica. 2013. PMID: 24371974 Croatian.
-
Proximal Tibial Cortex Transverse Distraction Facilitating Healing and Limb Salvage in Severe and Recalcitrant Diabetic Foot Ulcers.Clin Orthop Relat Res. 2020 Apr;478(4):836-851. doi: 10.1097/CORR.0000000000001075. Clin Orthop Relat Res. 2020. PMID: 31794478 Free PMC article.
Cited by
-
SFRP2 modulates functional phenotype transition and energy metabolism of macrophages during diabetic wound healing.Front Immunol. 2024 Oct 11;15:1432402. doi: 10.3389/fimmu.2024.1432402. eCollection 2024. Front Immunol. 2024. PMID: 39464880 Free PMC article.
-
Multifunctional combined drug-loaded nanofibrous dressings with anti-inflammatory, antioxidant stress and microenvironment improvement for diabetic wounds.RSC Adv. 2024 Sep 18;14(40):29606-29623. doi: 10.1039/d4ra04860a. eCollection 2024 Sep 12. RSC Adv. 2024. PMID: 39297039 Free PMC article.
-
Effect of Compound Xuejie Powder combined with negative pressure wound therapy on diabetic foot ulcers and blood flow in the dorsal foot artery.Am J Transl Res. 2024 Sep 15;16(9):4996-5003. doi: 10.62347/XSXY3749. eCollection 2024. Am J Transl Res. 2024. PMID: 39398571 Free PMC article.
-
A systematic review of diabetic foot infections: pathogenesis, diagnosis, and management strategies.Front Clin Diabetes Healthc. 2024 Aug 6;5:1393309. doi: 10.3389/fcdhc.2024.1393309. eCollection 2024. Front Clin Diabetes Healthc. 2024. PMID: 39165660 Free PMC article.
-
Antibacterial Activity and Mechanism of Canagliflozin against Methicillin-Resistant Staphylococcus aureus.Molecules. 2023 Jul 26;28(15):5668. doi: 10.3390/molecules28155668. Molecules. 2023. PMID: 37570637 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
