

Assessing respiratory viral exclusion and affinity interactions through co-infection incidence in a pediatric population during the 2022 resurgence of influenza and RSV
- PMID: 37389220
- PMCID: PMC10302716
- DOI: 10.3389/fcimb.2023.1208235
Assessing respiratory viral exclusion and affinity interactions through co-infection incidence in a pediatric population during the 2022 resurgence of influenza and RSV
Abstract
Introduction: In the Northeast US, respiratory viruses such as influenza and respiratory syncytial virus (RSV), which were largely suppressed by COVID-19-related social distancing, made an unprecedented resurgence during 2022, leading to a substantial rise in viral co-infections. However, the relative rates of co-infection with seasonal respiratory viruses over this period have not been assessed.
Methods: Here we reviewed multiplex respiratory viral PCR data (BioFire FilmArray™ Respiratory Panel v2.1 [RPP]) from patients with respiratory symptoms presenting to our medical center in New York City to assess co-infection rates of respiratory viruses, which were baselined to total rates of infection for each virus. We examined trends in monthly RPP data from adults and children during November 2021 through December 2022 to capture the full seasonal dynamics of respiratory viruses across periods of low and high prevalence.
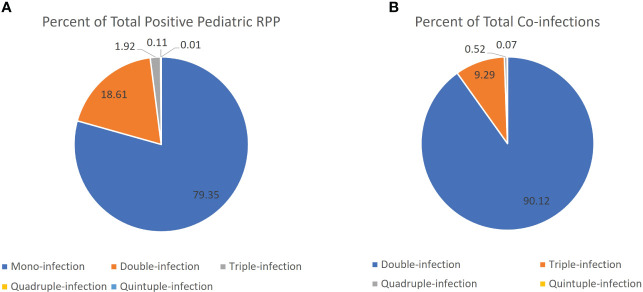
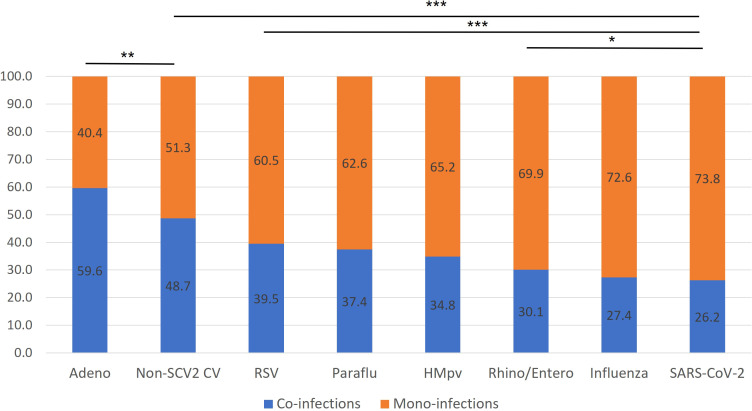
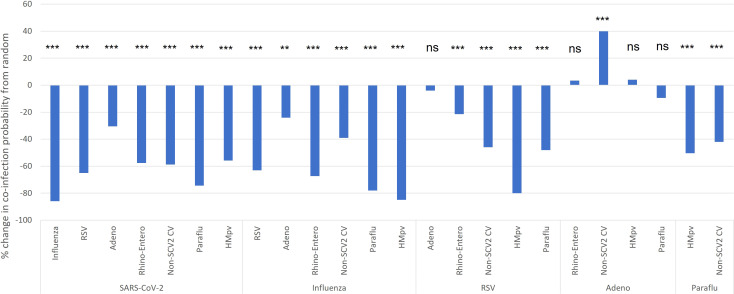
Results: Of 50,022 RPPs performed for 34,610 patients, 44% were positive for at least one target, and 67% of these were from children. The overwhelming majority of co-infections (93%) were seen among children, for whom 21% of positive RPPs had two or more viruses detected, as compared to just 4% in adults. Relative to children for whom RPPs were ordered, children with co-infections were younger (3.0 vs 4.5 years) and more likely to be seen in the ED or outpatient settings than inpatient and ICU settings. In children, most viral co-infections were found at significantly reduced rates relative to that expected from the incidence of each virus, especially those involving SARS-CoV-2 and influenza. SARS-CoV-2 positive children had an 85%, 65% and 58% reduced rate of co-infection with influenza, RSV, and Rhino/enteroviruses, respectively, after compensating for the incidence of infection with each virus (p< 0.001).
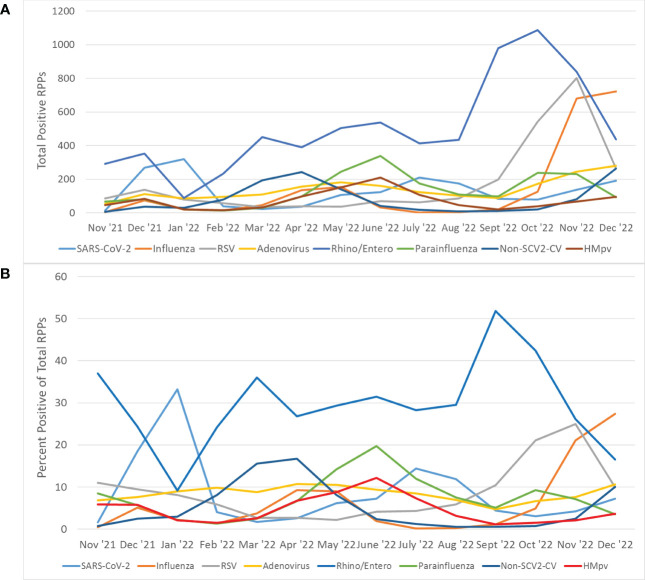
Discussion: Our results demonstrate that most respiratory viruses peaked in different months and present in co-infections less than would be expected based on overall rates of infection, suggesting a viral exclusionary effect between most seasonal respiratory viruses, including SARS-CoV-2, influenza and RSV. We also demonstrate the significant burden of respiratory viral co-infections among children. Further work is necessary to understand what predisposes certain patients for viral co-infection despite this exclusionary effect.
Keywords: COVID-19; RSV; SARS-CoV-2; co-infection; influenza; multiplex; respiratory; virus.
Copyright © 2023 Weidmann, Green, Berry and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Resurgence of influenza and respiratory syncytial virus in Egypt following two years of decline during the COVID-19 pandemic: outpatient clinic survey of infants and children, October 2022.BMC Public Health. 2023 Jun 5;23(1):1067. doi: 10.1186/s12889-023-15880-9. BMC Public Health. 2023. PMID: 37277781 Free PMC article.
-
Viral co-infection with human respiratory syncytial virus in suspected acute and severe respiratory tract infections during COVID-19 pandemic in Yaoundé, Cameroon, 2020-2021.Influenza Other Respir Viruses. 2023 Mar;17(3):e13131. doi: 10.1111/irv.13131. Influenza Other Respir Viruses. 2023. PMID: 36991539 Free PMC article.
-
A delayed resurgence of respiratory syncytial virus (RSV) during the COVID-19 pandemic: An unpredictable outbreak in a small proportion of children in the Southwest of Iran, April 2022.J Med Virol. 2022 Dec;94(12):5802-5807. doi: 10.1002/jmv.28065. Epub 2022 Aug 23. J Med Virol. 2022. PMID: 35961780 Free PMC article.
-
COVID-19 and Respiratory Virus Co-Infections: A Systematic Review of the Literature.Viruses. 2023 Mar 28;15(4):865. doi: 10.3390/v15040865. Viruses. 2023. PMID: 37112844 Free PMC article. Review.
-
Physical interventions to interrupt or reduce the spread of respiratory viruses.Cochrane Database Syst Rev. 2023 Jan 30;1(1):CD006207. doi: 10.1002/14651858.CD006207.pub6. Cochrane Database Syst Rev. 2023. PMID: 36715243 Free PMC article. Review.
Cited by
-
Clinical Evaluation of the BIOFIRE SPOTFIRE Respiratory Panel.Viruses. 2024 Apr 13;16(4):600. doi: 10.3390/v16040600. Viruses. 2024. PMID: 38675941 Free PMC article.
-
Diagnostic Accuracy of the LabTurbo QuadAIO Common Flu Assay for Detecting Influenza A Virus, Influenza B Virus, RSV, and SARS-CoV-2.Diagnostics (Basel). 2024 Oct 2;14(19):2200. doi: 10.3390/diagnostics14192200. Diagnostics (Basel). 2024. PMID: 39410604 Free PMC article.
-
Assessment of Antibiotic Resistance in Pediatric Infections: A Romanian Case Study on Pathogen Prevalence and Effective Treatments.Antibiotics (Basel). 2024 Sep 13;13(9):879. doi: 10.3390/antibiotics13090879. Antibiotics (Basel). 2024. PMID: 39335052 Free PMC article.
-
The Seasonality of Respiratory Viruses in a Hong Kong Hospital, 2014-2023.Viruses. 2023 Aug 26;15(9):1820. doi: 10.3390/v15091820. Viruses. 2023. PMID: 37766227 Free PMC article.
-
Differences in the Clinical Manifestations and Host Immune Responses to SARS-CoV-2 Variants in Children Compared to Adults.J Clin Med. 2023 Dec 26;13(1):128. doi: 10.3390/jcm13010128. J Clin Med. 2023. PMID: 38202135 Free PMC article. Review.
References
-
- Adams K., Tastad K. J., Huang S., Ujamaa D., Kniss K., Cummings C., et al. . (2022). Prevalence of SARS-CoV-2 and influenza coinfection and clinical characteristics among children and adolescents Aged<18 years who were hospitalized or died with influenza - united states, 2021-22 influenza season. MMWR Morb. Mortal Wkly. Rep. 71 (50), 1589–1596. doi: 10.15585/mmwr.mm7150a4 - DOI - PMC - PubMed
-
- Alhumaid S., Alabdulqader M., Al Dossary N., Al Alawi Z., Alnaim A. A., Al Mutared K. M., et al. . (2021). Coinfections with bacteria, fungi, and respiratory viruses in patients with SARS-CoV-2: a systematic review and meta-analysis. Pathogens 10 (7). doi: 10.3390/pathogens10070809 - DOI - PMC - PubMed
-
- Alhumaid S., Al Mutair A., Al Alawi Z., Alshawi A. M., Alomran S. A., Almuhanna M. S., et al. . (2022). Global coinfections with bacteria, fungi, and respiratory viruses in children with SARS-CoV-2: a systematic review and meta-analysis. Trop. Med. Infect. Dis. 7 (11). doi: 10.3390/tropicalmed7110380 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous