

Evaluating Metformin Strategies for Cancer Prevention: A Target Trial Emulation Using Electronic Health Records
- PMID: 37227368
- PMCID: PMC10524586
- DOI: 10.1097/EDE.0000000000001626
Evaluating Metformin Strategies for Cancer Prevention: A Target Trial Emulation Using Electronic Health Records
Abstract
Background: Metformin users appear to have a substantially lower risk of cancer than nonusers in many observational studies. These inverse associations may be explained by common flaws in observational analyses that can be avoided by explicitly emulating a target trial.
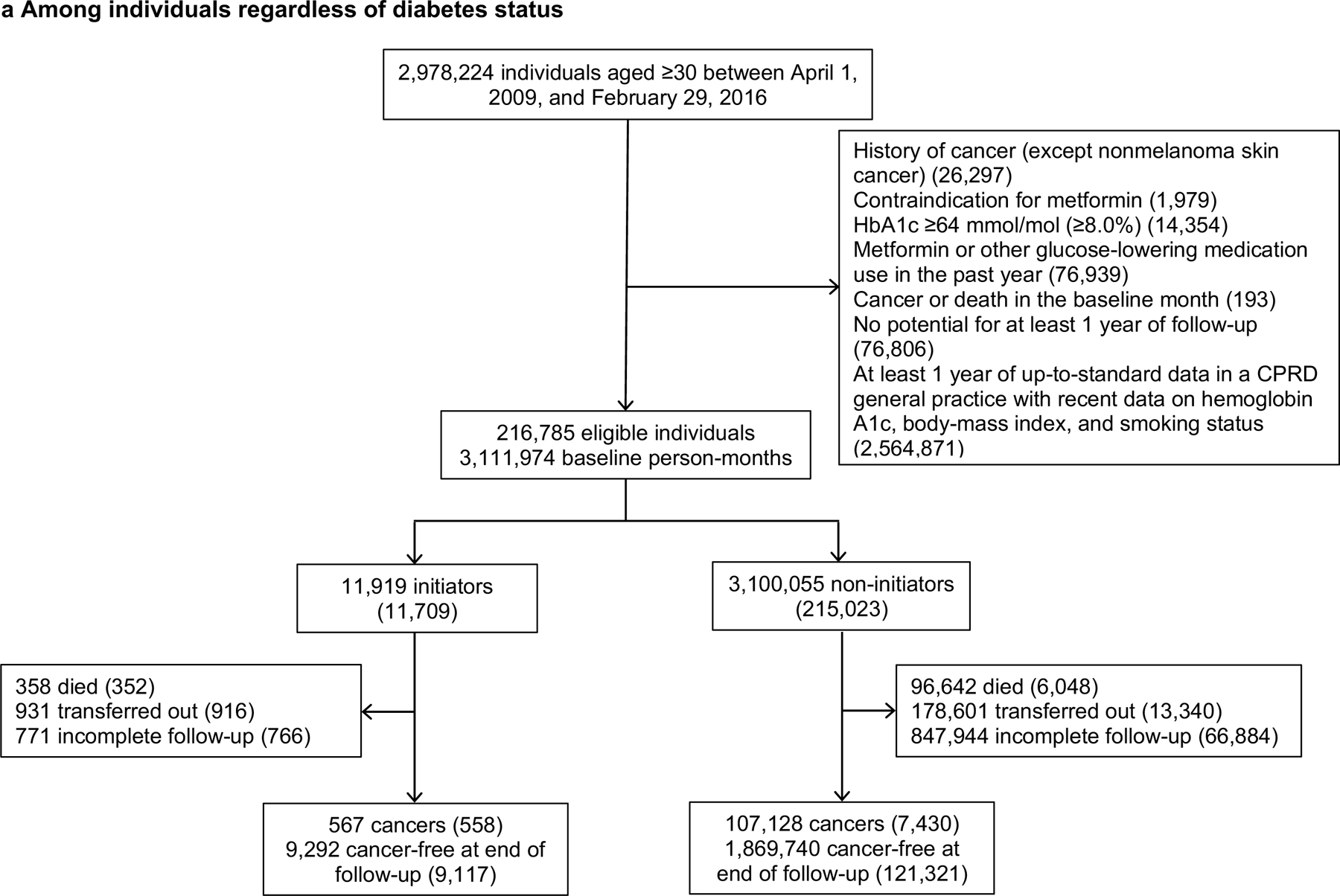
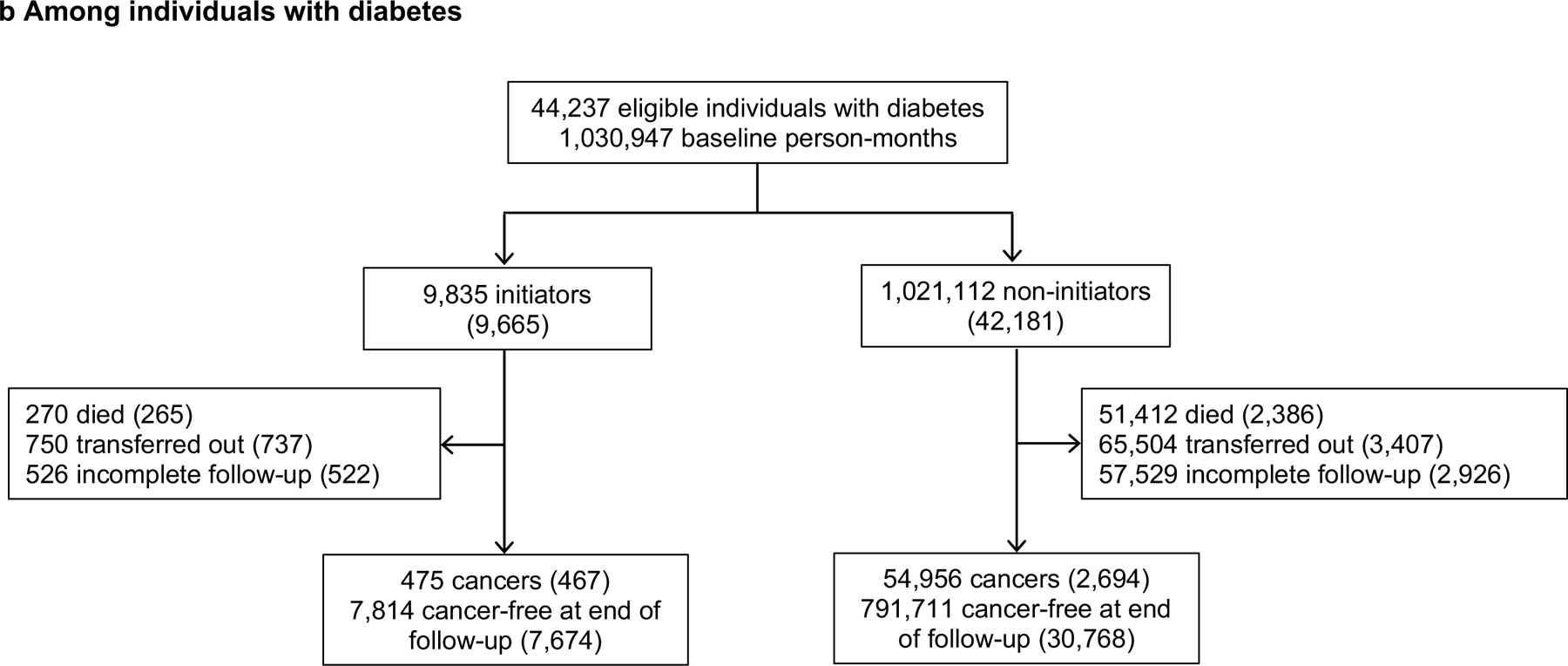
Methods: We emulated target trials of metformin therapy and cancer risk using population-based linked electronic health records from the UK (2009-2016). We included individuals with diabetes, no history of cancer, no recent prescription for metformin or other glucose-lowering medication, and hemoglobin A1c (HbA1c) <64 mmol/mol (<8.0%). Outcomes included total cancer and 4 site-specific cancers (breast, colorectal, lung, and prostate). We estimated risks using pooled logistic regression with adjustment for risk factors via inverse-probability weighting. We emulated a second target trial among individuals regardless of diabetes status. We compared our estimates with those obtained using previously applied analytic approaches.
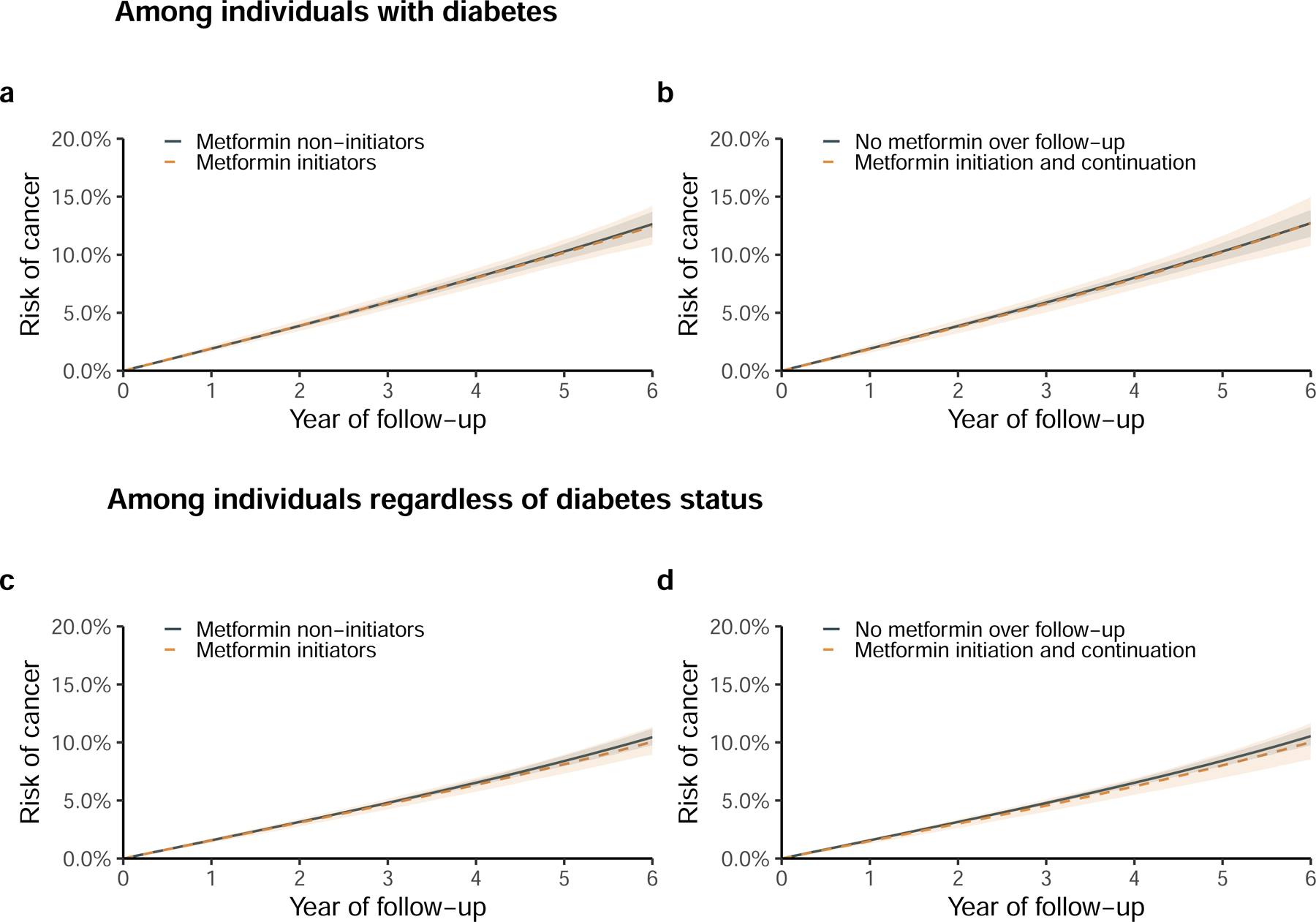
Results: Among individuals with diabetes, the estimated 6-year risk differences (metformin - no metformin) were -0.2% (95% CI = -1.6%, 1.3%) in the intention-to-treat analysis and 0.0% (95% CI = -2.1%, 2.3%) in the per-protocol analysis. The corresponding estimates for all site-specific cancers were close to zero. Among individuals regardless of diabetes status, these estimates were also close to zero and more precise. By contrast, previous analytic approaches yielded estimates that appeared strongly protective.
Conclusions: Our findings are consistent with the hypothesis that metformin therapy does not meaningfully influence cancer incidence. The findings highlight the importance of explicitly emulating a target trial to reduce bias in the effect estimates derived from observational analyses.
Copyright © 2023 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Comment in
-
Why is target trial emulation not being used in health technology assessment real-world data submissions?J Comp Eff Res. 2024 Aug;13(8):e240091. doi: 10.57264/cer-2024-0091. Epub 2024 Jun 8. J Comp Eff Res. 2024. PMID: 38850128 Free PMC article. No abstract available.
Similar articles
-
Metformin use and risk of cancer in patients with type 2 diabetes: a cohort study of primary care records using inverse probability weighting of marginal structural models.Int J Epidemiol. 2019 Apr 1;48(2):527-537. doi: 10.1093/ije/dyz005. Int J Epidemiol. 2019. PMID: 30753459 Free PMC article.
-
Avoidable flaws in observational analyses: an application to statins and cancer.Nat Med. 2019 Oct;25(10):1601-1606. doi: 10.1038/s41591-019-0597-x. Epub 2019 Oct 7. Nat Med. 2019. PMID: 31591592 Free PMC article.
-
Metformin for prevention or delay of type 2 diabetes mellitus and its associated complications in persons at increased risk for the development of type 2 diabetes mellitus.Cochrane Database Syst Rev. 2019 Dec 3;12(12):CD008558. doi: 10.1002/14651858.CD008558.pub2. Cochrane Database Syst Rev. 2019. PMID: 31794067 Free PMC article.
-
Dipeptidyl-peptidase (DPP)-4 inhibitors and glucagon-like peptide (GLP)-1 analogues for prevention or delay of type 2 diabetes mellitus and its associated complications in people at increased risk for the development of type 2 diabetes mellitus.Cochrane Database Syst Rev. 2017 May 10;5(5):CD012204. doi: 10.1002/14651858.CD012204.pub2. Cochrane Database Syst Rev. 2017. PMID: 28489279 Free PMC article. Review.
-
Insulin secretagogues for prevention or delay of type 2 diabetes mellitus and its associated complications in persons at increased risk for the development of type 2 diabetes mellitus.Cochrane Database Syst Rev. 2016 Oct 17;10(10):CD012151. doi: 10.1002/14651858.CD012151.pub2. Cochrane Database Syst Rev. 2016. PMID: 27749986 Free PMC article. Review.
Cited by
-
A Narrative Review: Repurposing Metformin as a Potential Therapeutic Agent for Oral Cancer.Cancers (Basel). 2024 Aug 29;16(17):3017. doi: 10.3390/cancers16173017. Cancers (Basel). 2024. PMID: 39272875 Free PMC article. Review.
-
Metformin and other anti-diabetic medication use and breast cancer incidence in the Nurses' Health Studies.Int J Cancer. 2024 Jul 15;155(2):211-225. doi: 10.1002/ijc.34917. Epub 2024 Mar 22. Int J Cancer. 2024. PMID: 38520039
-
Patients with oral tongue squamous cell carcinoma and co‑existing diabetes exhibit lower recurrence rates and improved survival: Implications for treatment.Oncol Lett. 2024 Feb 6;27(4):142. doi: 10.3892/ol.2024.14275. eCollection 2024 Apr. Oncol Lett. 2024. PMID: 38385115 Free PMC article.
-
Does metformin really reduce prostate cancer risk: an up-to-date comprehensive genome-wide analysis.Diabetol Metab Syndr. 2024 Jul 12;16(1):159. doi: 10.1186/s13098-024-01397-7. Diabetol Metab Syndr. 2024. PMID: 38997745 Free PMC article.
-
Why is target trial emulation not being used in health technology assessment real-world data submissions?J Comp Eff Res. 2024 Aug;13(8):e240091. doi: 10.57264/cer-2024-0091. Epub 2024 Jun 8. J Comp Eff Res. 2024. PMID: 38850128 Free PMC article. No abstract available.
References
-
- Chikermane SG, Sharma M, Abughosh SM, Aparasu RR, Trivedi MV, Johnson ML. Dose-dependent relation between metformin and the risk of hormone receptor-positive, her2-negative breast cancer among postmenopausal women with type-2 diabetes. Breast Cancer Res Treat 2022;195(3):421–430. - PubMed
-
- Lee JW, Choi EA, Kim YS, et al. Metformin usage and the risk of colorectal cancer: a national cohort study. Int J Colorectal Dis 2021;36(2):303–310. - PubMed
-
- Zhang ZJ, Bi Y, Li S, et al. Reduced risk of lung cancer with metformin therapy in diabetic patients: a systematic review and meta-analysis. Am J Epidemiol 2014;180(1):11–14. - PubMed
-
- Col NF, Ochs L, Springmann V, Aragaki AK, Chlebowski RT. Metformin and breast cancer risk: a meta-analysis and critical literature review. Breast Cancer Res Treat 2012;135(3):639–646. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
