

Using Continuous Glucose Monitoring to Prescribe a Time to Exercise for Individuals with Type 2 Diabetes
- PMID: 37176677
- PMCID: PMC10179271
- DOI: 10.3390/jcm12093237
Using Continuous Glucose Monitoring to Prescribe a Time to Exercise for Individuals with Type 2 Diabetes
Abstract
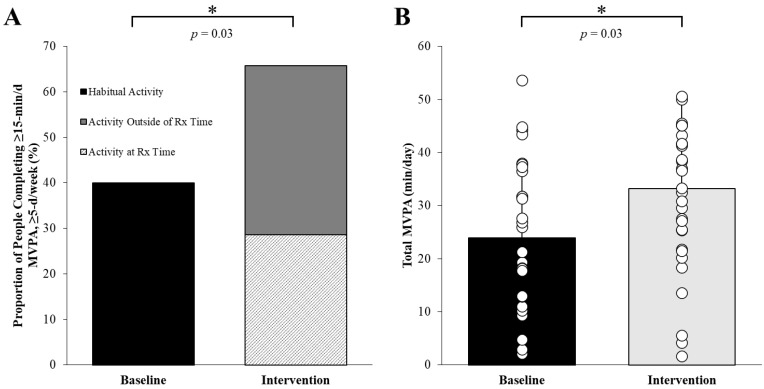
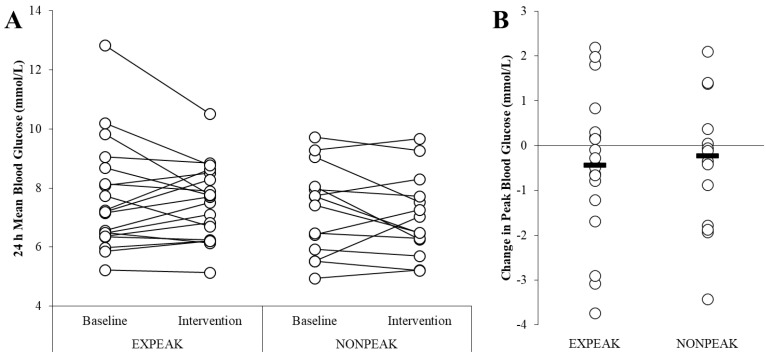
This study examines the potential utility of using continuous glucose monitoring (CGM) to prescribe an exercise time to target peak hyperglycaemia in people with type 2 diabetes (T2D). The main aim is to test the feasibility of prescribing an individualised daily exercise time, based on the time of CGM-derived peak glucose, for people with T2D. Thirty-five individuals with T2D (HbA1c: 7.2 ± 0.8%; age: 64 ± 7 y; BMI: 29.2 ± 5.2 kg/m2) were recruited and randomised to one of two 14 d exercise interventions: i) ExPeak (daily exercise starting 30 min before peak hyperglycaemia) or placebo active control NonPeak (daily exercise starting 90 min after peak hyperglycaemia). The time of peak hyperglycaemia was determined via a two-week baseline CGM. A CGM, accelerometer, and heart rate monitor were worn during the free-living interventions to objectively measure glycaemic control outcomes, moderate-to-vigorous intensity physical activity (MVPA), and exercise adherence for future translation in a clinical trial. Participation in MVPA increased 26% when an exercise time was prescribed compared to habitual baseline (p < 0.01), with no difference between intervention groups (p > 0.26). The total MVPA increased by 10 min/day during the intervention compared to the baseline (baseline: 23 ± 14 min/d vs. intervention: 33 ± 16 min/d, main effect of time p = 0.03, no interaction). The change in peak blood glucose (mmol/L) was similar between the ExPeak (-0.44 ± 1.6 mmol/L, d = 0.21) and the NonPeak (-0.39 ± 1.5 mmol/L, d = 0.16) intervention groups (p = 0.92). Prescribing an exercise time based on CGM may increase daily participation in physical activity in people with type 2 diabetes; however, further studies are needed to test the long-term impact of this approach.
Keywords: continuous glucose monitoring; hyperglycaemia; physical activity; prescribed exercise timing; type 2 diabetes.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Personalising activity to target peak hyperglycaemia and improve cardiometabolic health in people with type 2 diabetes: protocol for a randomised controlled trial.BMJ Open. 2022 Mar 29;12(3):e057183. doi: 10.1136/bmjopen-2021-057183. BMJ Open. 2022. PMID: 35351723 Free PMC article.
-
Effect of initiating use of an insulin pump in adults with type 1 diabetes using multiple daily insulin injections and continuous glucose monitoring (DIAMOND): a multicentre, randomised controlled trial.Lancet Diabetes Endocrinol. 2017 Sep;5(9):700-708. doi: 10.1016/S2213-8587(17)30217-6. Epub 2017 Jul 12. Lancet Diabetes Endocrinol. 2017. PMID: 28711468 Clinical Trial.
-
Behavioural interventions to promote physical activity in a multiethnic population at high risk of diabetes: PROPELS three-arm RCT.Health Technol Assess. 2021 Dec;25(77):1-190. doi: 10.3310/hta25770. Health Technol Assess. 2021. PMID: 34995176 Clinical Trial.
-
Diabetes technology and treatments in the paediatric age group.Int J Clin Pract Suppl. 2011 Feb;(170):76-82. doi: 10.1111/j.1742-1241.2010.02582.x. Int J Clin Pract Suppl. 2011. PMID: 21323816 Review.
-
FreeStyle Libre Flash Glucose Self-Monitoring System: A Single-Technology Assessment [Internet].Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Aug 21. Report from the Norwegian Institute of Public Health No. 2017-07. Oslo, Norway: Knowledge Centre for the Health Services at The Norwegian Institute of Public Health (NIPH); 2017 Aug 21. Report from the Norwegian Institute of Public Health No. 2017-07. PMID: 29553668 Free Books & Documents. Review.
Cited by
-
Exercise Prescription for Postprandial Glycemic Management.Nutrients. 2024 Apr 14;16(8):1170. doi: 10.3390/nu16081170. Nutrients. 2024. PMID: 38674861 Free PMC article. Review.
References
-
- Bull F.C., Al-Ansari S.S., Biddle S., Borodulin K., Buman M.P., Cardon G., Carty C., Chaput J.-P., Chastin S., Chou R., et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020;54:1451–1462. doi: 10.1136/bjsports-2020-102955. - DOI - PMC - PubMed
-
- IDF Diabetes Atlas. 10th ed. International Diabetes Federation; Brussels, Belgium: 2021.
-
- Jarvie J.L., Pandey A., Ayers C.R., McGavock J.M., Sénéchal M., Berry J.D., Patel K.V., McGuire D.K. Aerobic fitness and adherence to guideline-recommended minimum physical activity among ambulatory patients with type 2 diabetes mellitus. Diabetes Care. 2019;42:1333–1339. doi: 10.2337/dc18-2634. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
