

SGK1 inhibition attenuated the action potential duration in patient- and genotype-specific re-engineered heart cells with congenital long QT syndrome
- PMID: 37124559
- PMCID: PMC10134391
- DOI: 10.1016/j.hroo.2023.02.003
SGK1 inhibition attenuated the action potential duration in patient- and genotype-specific re-engineered heart cells with congenital long QT syndrome
Abstract
Background: Long QT syndrome (LQTS) stems from pathogenic variants in KCNQ1 (LQT1), KCNH2 (LQT2), or SCN5A (LQT3) and is characterized by action potential duration (APD) prolongation. Inhibition of serum and glucocorticoid regulated kinase-1 (SGK1) is proposed as a novel therapeutic for LQTS.
Objective: The study sought to test the efficacy of novel, selective SGK1 inhibitors in induced pluripotent stem cell-derived cardiomyocyte (iPSC-CM) models of LQTS.
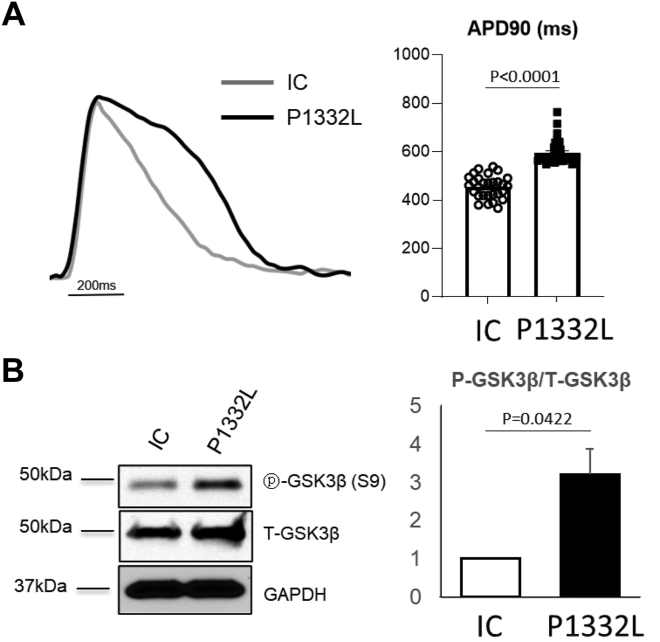
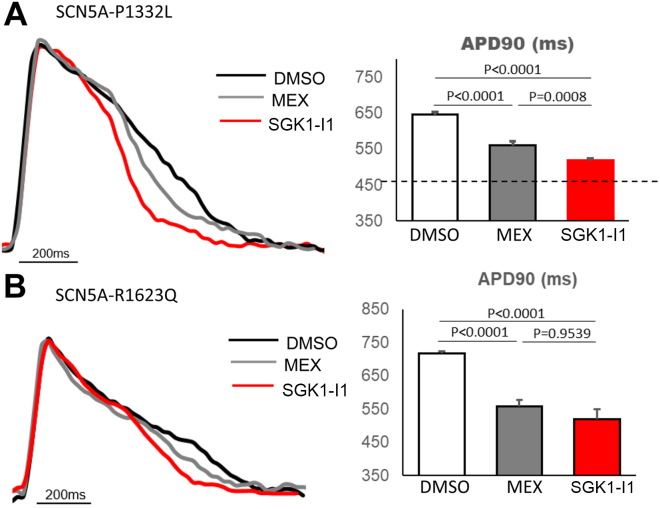
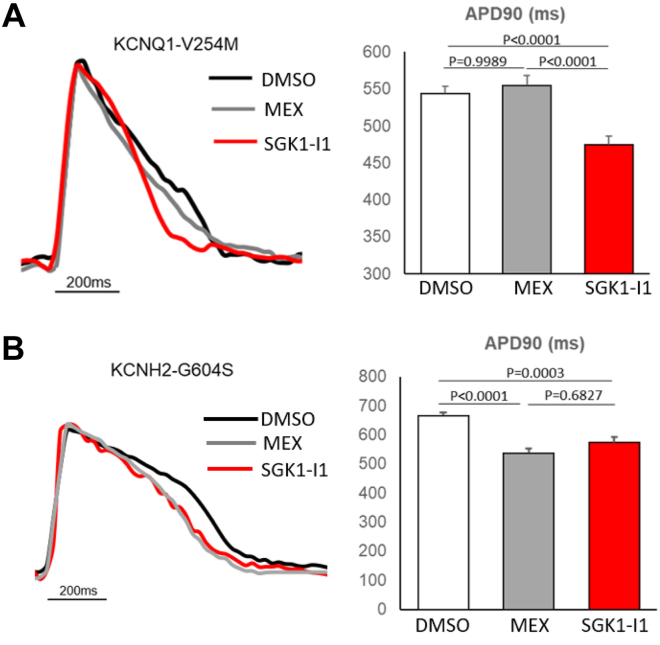
Methods: The mexiletine (MEX)-sensitive SCN5A-P1332L iPSC-CMs were tested initially compared with a CRISPR (clustered regularly interspaced short palindromic repeats)/Cas9 SCN5A-P1332L variant-corrected isogenic control (IC). The SGK1-I1 therapeutic efficacy, compared with MEX, was tested for APD at 90% repolarization (APD90) shortening in SCN5A-P1332L, SCN5A-R1623Q, KCNH2-G604S, and KCNQ1-V254M iPSC-CMs using FluoVolt.
Results: The APD90 was prolonged in SCN5A-P1332L iPSC-CMs compared with its IC (646 ± 7 ms vs 482 ± 23 ms; P < .0001). MEX shortened the APD90 to 560 ± 7 ms (52% attenuation, P < .0001). SGK1-I1 shortened the APD90 to 518 ± 5 ms (78% attenuation, P < .0001) but did not shorten the APD90 in the IC. SGK1-I1 shortened the APD90 of the SCN5A-R1623Q iPSC-CMs (753 ± 8 ms to 475 ± 19 ms compared with 558 ± 19 ms with MEX), the KCNH2-G604S iPSC-CMs (666 ± 10 ms to 574 ± 18 ms vs 538 ± 15 ms after MEX), and the KCNQ1-V254M iPSC-CMs (544 ± 10 ms to 475 ± 11ms; P = .0004).
Conclusions: Therapeutically inhibiting SGK1 effectively shortens the APD in human iPSC-CM models of the 3 major LQTS genotypes. These preclinical data support development of SGK1 inhibitors as novel, first-in-class therapy for patients with congenital LQTS.
Keywords: Long QT syndrome; SGK1; Serum and glucocorticoid regulated kinase-1; Therapeutic; Treatment; iPSC.
© 2023 Heart Rhythm Society. Published by Elsevier Inc.
Figures
Similar articles
-
Gene- and variant-specific efficacy of serum/glucocorticoid-regulated kinase 1 inhibition in long QT syndrome types 1 and 2.Europace. 2023 May 19;25(5):euad094. doi: 10.1093/europace/euad094. Europace. 2023. PMID: 37099628 Free PMC article.
-
SGK1 inhibition attenuates the action potential duration in reengineered heart cell models of drug-induced QT prolongation.Heart Rhythm. 2023 Apr;20(4):589-595. doi: 10.1016/j.hrthm.2022.12.036. Epub 2023 Jan 5. Heart Rhythm. 2023. PMID: 36610526
-
Genome sequencing in a genetically elusive multigenerational long QT syndrome pedigree identifies a novel LQT2-causative deeply intronic KCNH2 variant.Heart Rhythm. 2022 Jun;19(6):998-1007. doi: 10.1016/j.hrthm.2022.02.004. Epub 2022 Feb 7. Heart Rhythm. 2022. PMID: 35144019
-
Molecular biology of the long QT syndrome: impact on management.Pacing Clin Electrophysiol. 1997 Aug;20(8 Pt 2):2052-7. doi: 10.1111/j.1540-8159.1997.tb03626.x. Pacing Clin Electrophysiol. 1997. PMID: 9272507 Review.
-
Sodium channel blockers in the management of long QT syndrome types 3 and 2: A system review and meta-analysis.J Cardiovasc Electrophysiol. 2021 Nov;32(11):3057-3067. doi: 10.1111/jce.15223. Epub 2021 Sep 1. J Cardiovasc Electrophysiol. 2021. PMID: 34427958 Review.
Cited by
-
Gene- and variant-specific efficacy of serum/glucocorticoid-regulated kinase 1 inhibition in long QT syndrome types 1 and 2.Europace. 2023 May 19;25(5):euad094. doi: 10.1093/europace/euad094. Europace. 2023. PMID: 37099628 Free PMC article.
-
Proof of concept for monoclonal antibody therapy in a cellular model of acquired long QT syndrome type 3.Am J Physiol Heart Circ Physiol. 2024 Jan 1;326(1):H89-H95. doi: 10.1152/ajpheart.00628.2023. Epub 2023 Nov 10. Am J Physiol Heart Circ Physiol. 2024. PMID: 37947435 Free PMC article.
References
-
- Ackerman M.J. Cardiac channelopathies: it's in the genes. Nat Med. 2004;10:463–464. - PubMed
-
- Rohatgi R.K., Sugrue A., Bos J.M., et al. Contemporary outcomes in patients with long QT syndrome. J Am Coll Cardiol. 2017;70:453–462. - PubMed
-
- Krøll J., Butt J.H., Jensen H.K., et al. β-blocker adherence among patients with congenital Long QT Syndrome: a nationwide study. Eur Heart J Qual Care Clin Outcomes. 2022;9:76–84. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
