

Total escape of SARS-CoV-2 from dual monoclonal antibody therapy in an immunocompromised patient
- PMID: 37037847
- PMCID: PMC10085998
- DOI: 10.1038/s41467-023-37591-w
Total escape of SARS-CoV-2 from dual monoclonal antibody therapy in an immunocompromised patient
Abstract
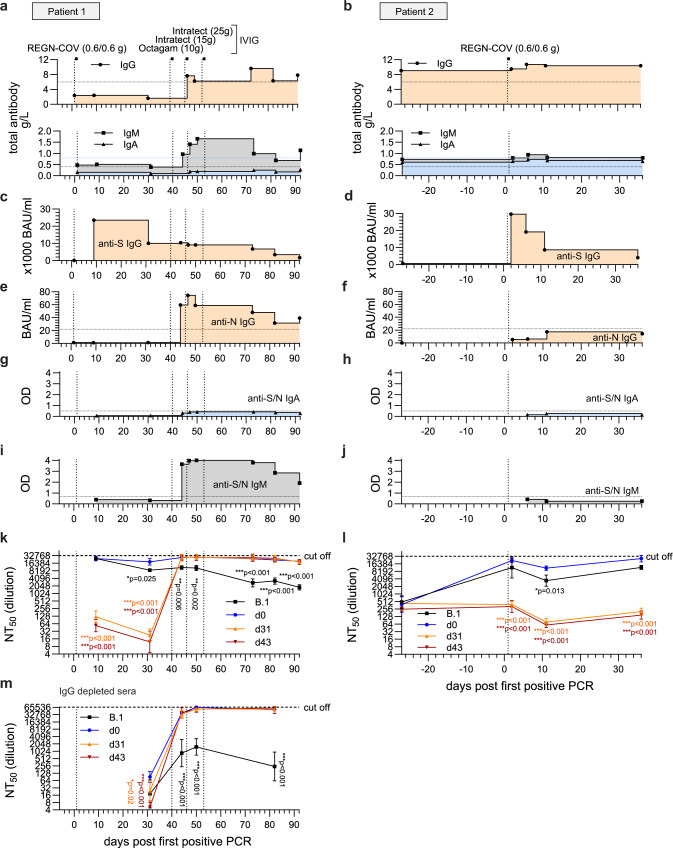
Monoclonal antibodies (mAbs) directed against the spike of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are effective therapeutic options to combat infections in high-risk patients. Here, we report the adaptation of SARS-CoV-2 to the mAb cocktail REGN-COV in a kidney transplant patient with hypogammaglobulinemia. Following mAb treatment, the patient did not clear the infection. During viral persistence, SARS-CoV-2 acquired three novel spike mutations. Neutralization and mouse protection analyses demonstrate a complete viral escape from REGN-COV at the expense of ACE-2 binding. Final clearance of the virus occurred upon reduction of the immunosuppressive regimen and total IgG substitution. Serology suggests that the development of highly neutralizing IgM rather than IgG substitution aids clearance. Our findings emphasise that selection pressure by mAbs on SARS-CoV-2 can lead to development of escape variants in immunocompromised patients. Thus, modification of immunosuppressive therapy, if possible, might be preferable to control and clearance of the viral infection.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Emergence of Multiple SARS-CoV-2 Antibody Escape Variants in an Immunocompromised Host Undergoing Convalescent Plasma Treatment.mSphere. 2021 Aug 25;6(4):e0048021. doi: 10.1128/mSphere.00480-21. Epub 2021 Aug 25. mSphere. 2021. PMID: 34431691 Free PMC article.
-
A Robust Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2)-Specific T- and B-Cell Response Is Associated With Early Viral Clearance in SARS-CoV-2 Omicron-Infected Immunocompromised Individuals.J Infect Dis. 2024 Oct 16;230(4):e860-e871. doi: 10.1093/infdis/jiae306. J Infect Dis. 2024. PMID: 38843052 Free PMC article.
-
Characterization of MW06, a human monoclonal antibody with cross-neutralization activity against both SARS-CoV-2 and SARS-CoV.MAbs. 2021 Jan-Dec;13(1):1953683. doi: 10.1080/19420862.2021.1953683. MAbs. 2021. PMID: 34313527 Free PMC article.
-
SARS-CoV-2 Neutralizing Antibodies for COVID-19 Prevention and Treatment.Annu Rev Med. 2022 Jan 27;73:1-16. doi: 10.1146/annurev-med-042420-113838. Epub 2021 Aug 24. Annu Rev Med. 2022. PMID: 34428080 Review.
-
Neutralizing monoclonal antibodies for the treatment and prophylaxis of SARS-CoV-2 infection.New Microbiol. 2021 Jul;44(3):135-144. New Microbiol. 2021. PMID: 34783348 Review.
Cited by
-
Influenza A virus resistance to 4'-fluorouridine coincides with viral attenuation in vitro and in vivo.PLoS Pathog. 2024 Feb 1;20(2):e1011993. doi: 10.1371/journal.ppat.1011993. eCollection 2024 Feb. PLoS Pathog. 2024. PMID: 38300953 Free PMC article.
-
Clinical phenotype and outcome of persistent SARS-CoV-2 replication in immunocompromised hosts: a retrospective observational study in the Omicron era.Infection. 2024 Jun;52(3):923-933. doi: 10.1007/s15010-023-02138-0. Epub 2023 Dec 14. Infection. 2024. PMID: 38095753 Free PMC article.
-
SARS-CoV-2 Variants from Long-Term, Persistently Infected Immunocompromised Patients Have Altered Syncytia Formation, Temperature-Dependent Replication, and Serum Neutralizing Antibody Escape.Viruses. 2024 Sep 9;16(9):1436. doi: 10.3390/v16091436. Viruses. 2024. PMID: 39339912 Free PMC article.
-
SARS-CoV-2 resistance to monoclonal antibodies and small-molecule drugs.Cell Chem Biol. 2024 Apr 18;31(4):632-657. doi: 10.1016/j.chembiol.2024.03.008. Cell Chem Biol. 2024. PMID: 38640902 Review.
-
Application of a Receptor-Binding-Domain-Based Simple Immunoassay for Assessing Humoral Immunity against Emerging SARS-CoV-2 Virus Variants.Biomedicines. 2023 Dec 1;11(12):3193. doi: 10.3390/biomedicines11123193. Biomedicines. 2023. PMID: 38137414 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
