

The Effect of Upper Cervical Mobilization/Manipulation on Temporomandibular Joint Pain, Maximal Mouth Opening, and Pressure Pain Thresholds: A Systematic Review and Meta-Analysis
- PMID: 36968167
- PMCID: PMC10036235
- DOI: 10.1016/j.arrct.2022.100242
The Effect of Upper Cervical Mobilization/Manipulation on Temporomandibular Joint Pain, Maximal Mouth Opening, and Pressure Pain Thresholds: A Systematic Review and Meta-Analysis
Abstract
Objective: To evaluate the efficacy of upper cervical joint mobilization and/or manipulation on reducing pain and improving maximal mouth opening (MMO) and pressure pain thresholds (PPTs) in adults with temporomandibular joint (TMJ) dysfunction compared with sham or other intervention.
Data sources: MEDLINE, CINAHL, EMBASE, and Cochrane Library from inception to June 3, 2022, were searched.
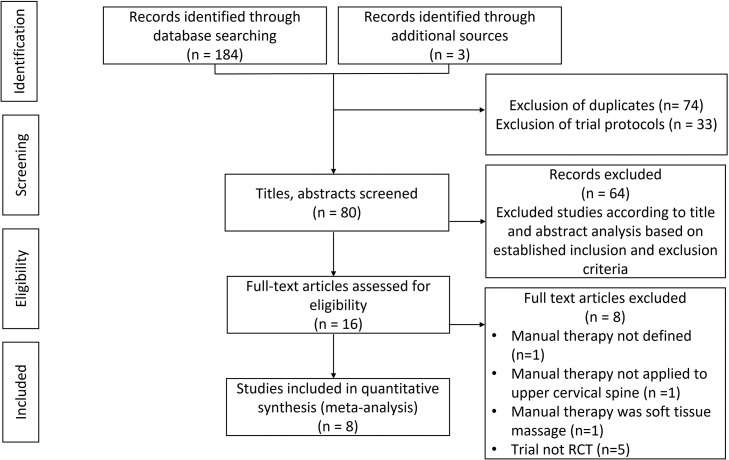
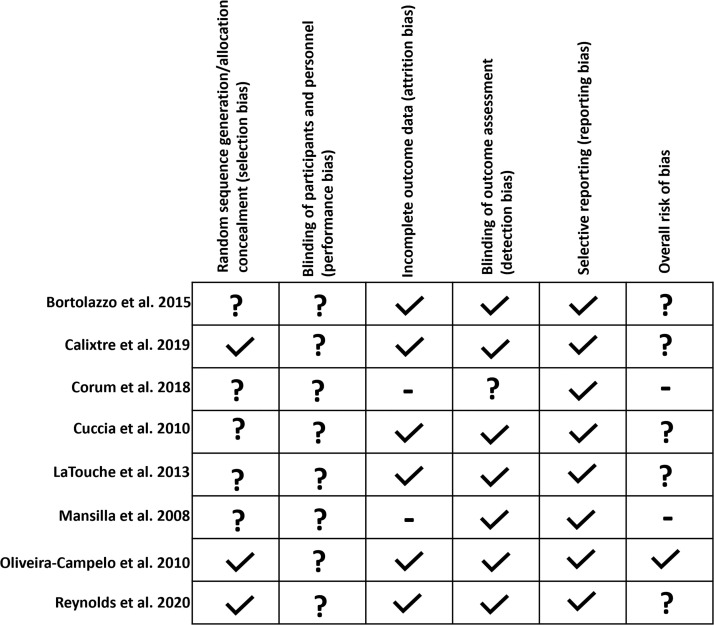
Study selection: Eight randomized controlled trials with 437 participants evaluating manual therapy (MT) vs sham and MT vs other intervention were included. Two reviewers independently extracted data and assessed risk of bias.
Data extraction: Two independent reviewers extracted information about origin, number of study participants, eligibility criteria, type of intervention, and outcome measures.
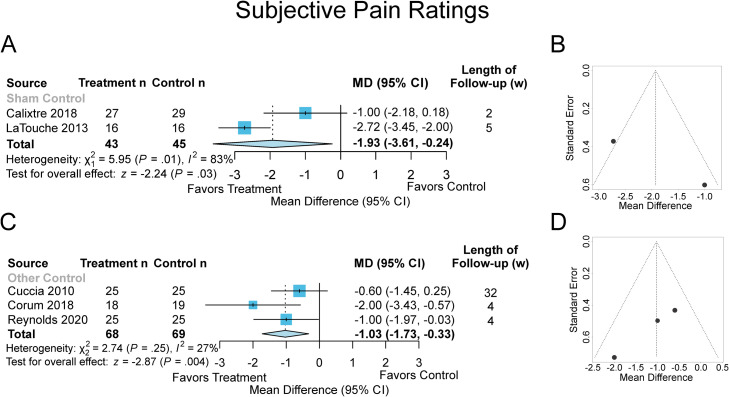
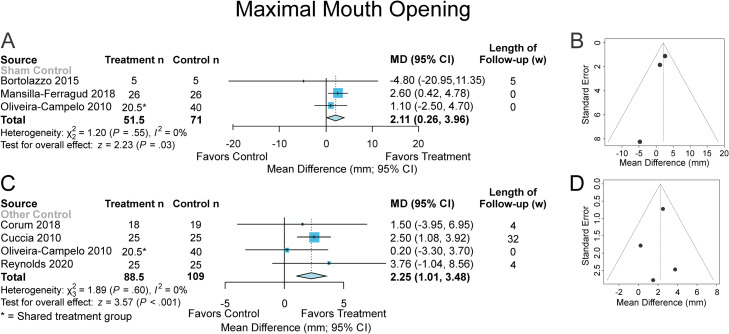
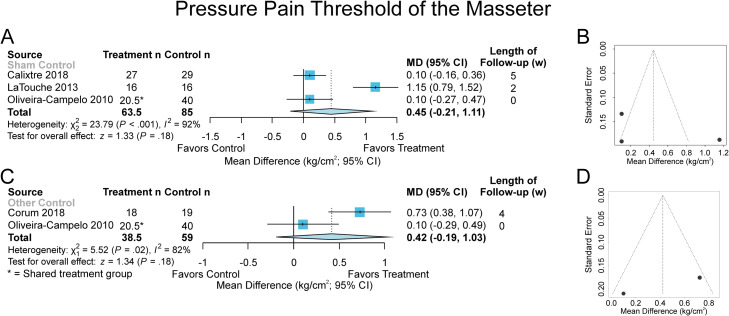
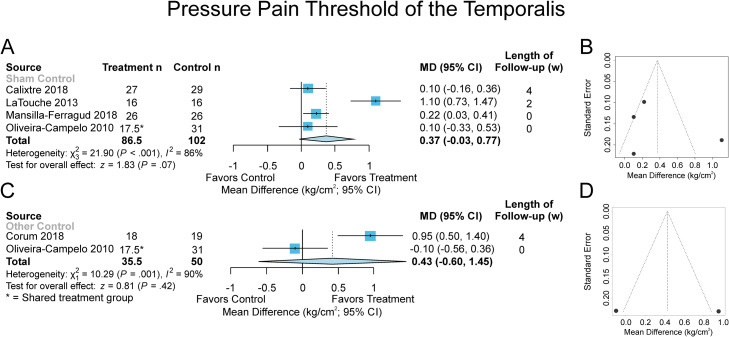
Data synthesis: Manual therapy was statistically significant in reducing pain compared with sham (mean difference [MD]: -1.93 points, 95% confidence interval [CI]: -3.61 to -0.24, P=.03), and other intervention (MD: -1.03 points, 95% CI: -1.73 to -0.33, P=.004), improved MMO compared with sham (MD: 2.11 mm, 95% CI: 0.26 to 3.96, P=.03), and other intervention (MD: 2.25 mm, 95% CI: 1.01 to 3.48, P<.001), but not statistically significant in improving PPT of masseter compared with sham (MD: 0.45 kg/cm2, 95% CI: -0.21 to 1.11, P=.18), and other intervention (MD: 0.42 kg/cm2, 95% CI: -0.19 to 1.03, P=.18), or the PPT of temporalis compared with sham (MD: 0.37 kg/cm2, 95% CI: -0.03 to 0.77, P=.07), and other intervention (MD: 0.43 kg/cm2, 95% CI: -0.60 to 1.45, P=.42).
Conclusion: There appears to be limited benefit of upper cervical spine MT on TMJ dysfunction, but definitive conclusions cannot be made because of heterogeneity and imprecision of treatment effects.
Keywords: Cervical vertebrae; Manipulation, spinal; Meta-analysis; Musculoskeletal manipulations; Pain; Rehabilitation; Systematic review; Temporomandibular joint.
© 2022 The Authors.
Figures
Similar articles
-
The effectiveness of cervical rehabilitation interventions for pain in adults with myogenic temporomandibular disorders: A systematic review and meta-analysis.J Oral Rehabil. 2024 Jun;51(6):1091-1107. doi: 10.1111/joor.13671. Epub 2024 Mar 7. J Oral Rehabil. 2024. PMID: 38454576
-
Effect of Manual Therapy and Therapeutic Exercise Applied to the Cervical Region on Pain and Pressure Pain Sensitivity in Patients with Temporomandibular Disorders: A Systematic Review and Meta-analysis.Pain Med. 2020 Oct 1;21(10):2373-2384. doi: 10.1093/pm/pnaa021. Pain Med. 2020. PMID: 32181811
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Manual therapy for the management of pain and limited range of motion in subjects with signs and symptoms of temporomandibular disorder: a systematic review of randomised controlled trials.J Oral Rehabil. 2015 Nov;42(11):847-61. doi: 10.1111/joor.12321. Epub 2015 Jun 7. J Oral Rehabil. 2015. PMID: 26059857 Review.
-
Complementary and alternative therapies for back pain II.Evid Rep Technol Assess (Full Rep). 2010 Oct;(194):1-764. Evid Rep Technol Assess (Full Rep). 2010. PMID: 23126534 Free PMC article. Review.
Cited by
-
Temporomandibular Disorders Management-What's New? A Scoping Review.Dent J (Basel). 2024 May 23;12(6):157. doi: 10.3390/dj12060157. Dent J (Basel). 2024. PMID: 38920858 Free PMC article.
References
-
- Greene CS, Klasser GD, Epstein JB. Revision of the American Association of Dental Research's science information statement about temporomandibular disorders. J Can Dent Assoc. 2010;76:a115. - PubMed
-
- Cooper BC, Kleinberg I. Examination of a large patient population for the presence of symptoms and signs of temporomandibular disorders. Cranio. 2007;25:114–126. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
