

Postponing colonoscopy for 6 months in high-risk population increases colorectal cancer detection in China
- PMID: 36951442
- PMCID: PMC10242305
- DOI: 10.1002/cam4.5850
Postponing colonoscopy for 6 months in high-risk population increases colorectal cancer detection in China
Abstract
Background and aims: Colonoscopy is an important colorectal cancer (CRC) screening modality; however, not all high-risk groups identified by fecal immunochemical test (FIT) and/or high-risk factor questionnaire (HRFQ) undergo colonoscopy in time. The impact of delays in colonoscopy on CRC detection among high-risk populations remains poorly understood, warranting further clarification.
Methods: A retrospective study was conducted among CRC high-risk population identified by Tianjin CRC screening program. According to the colonoscopy results after HRFQ and FIT, patients were classified into CRC, advanced adenoma, non-advanced adenoma, and normal groups. The time interval between CRC screening and colonoscopy was investigated and its relationship with colonoscopy results. Logistic regression was performed to explore the risk factors of CRC detection.
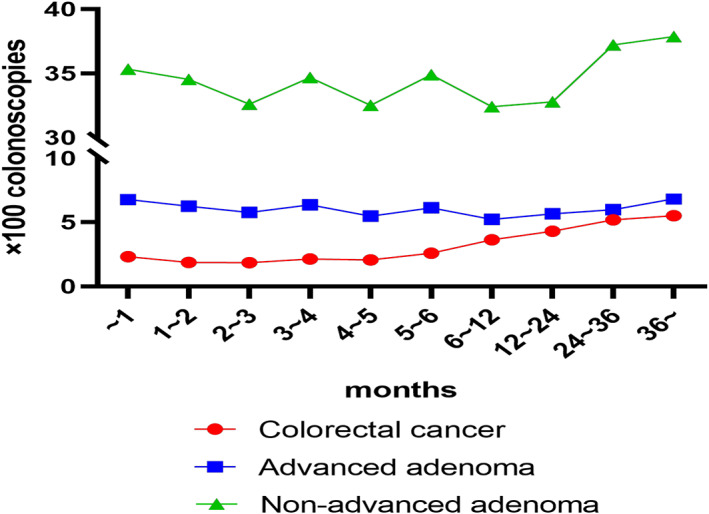
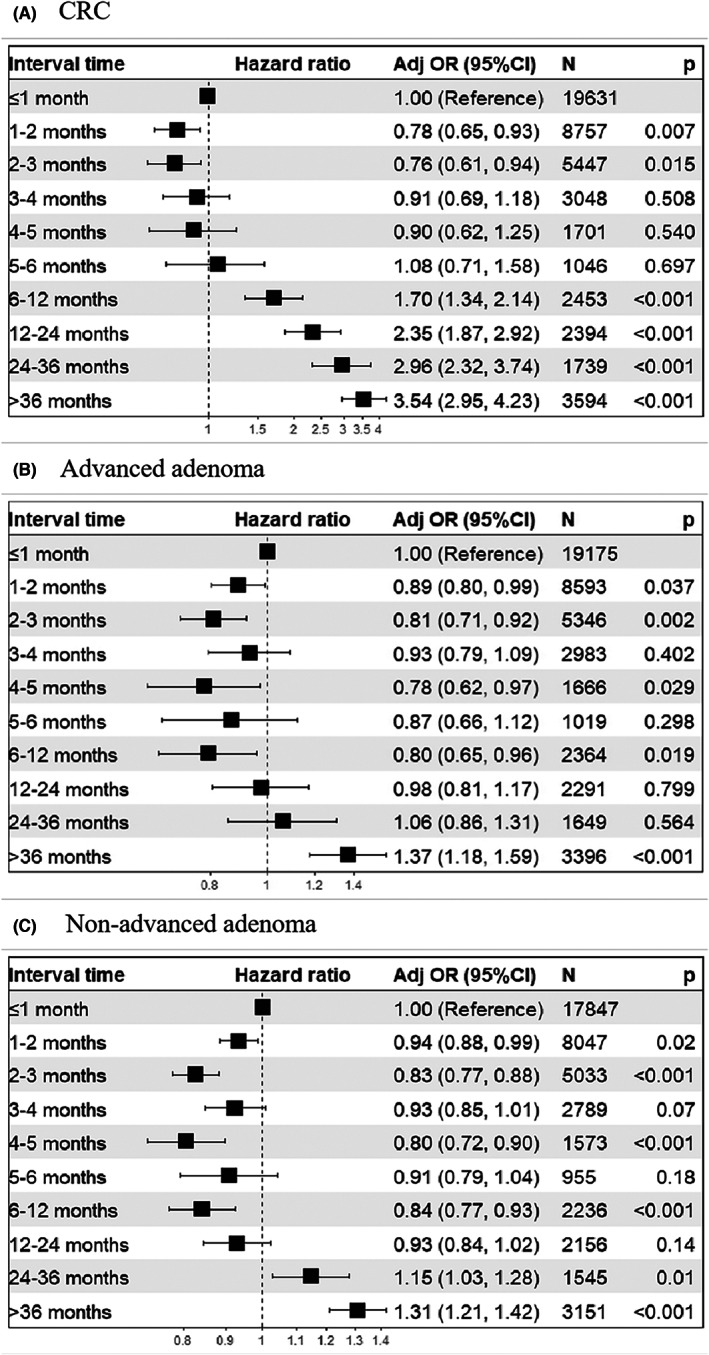
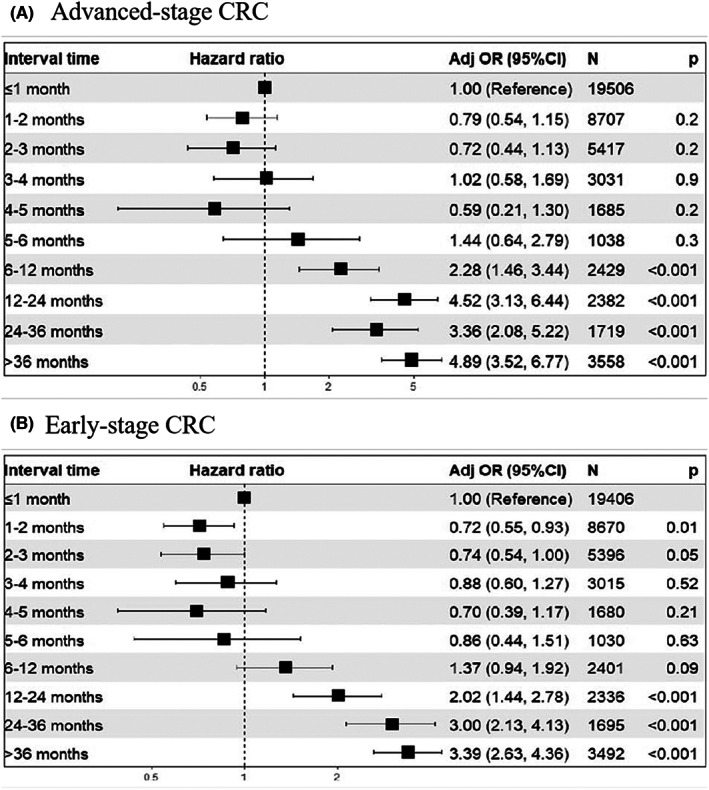
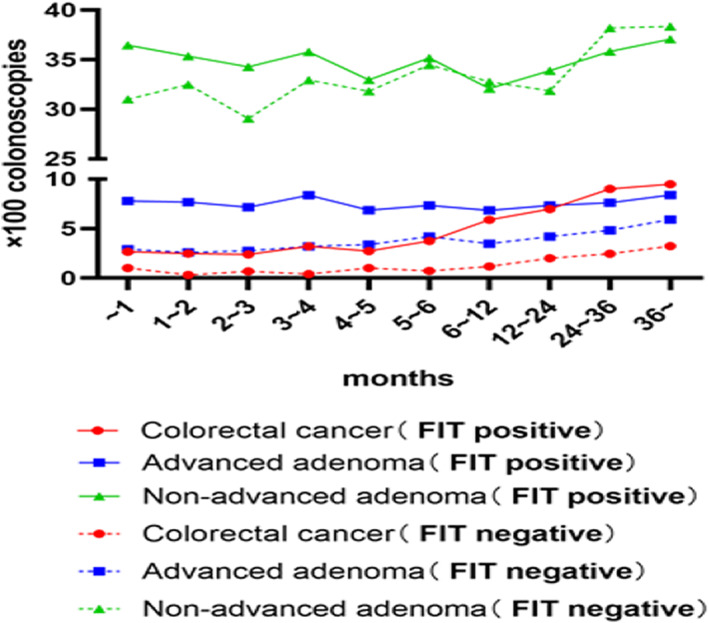
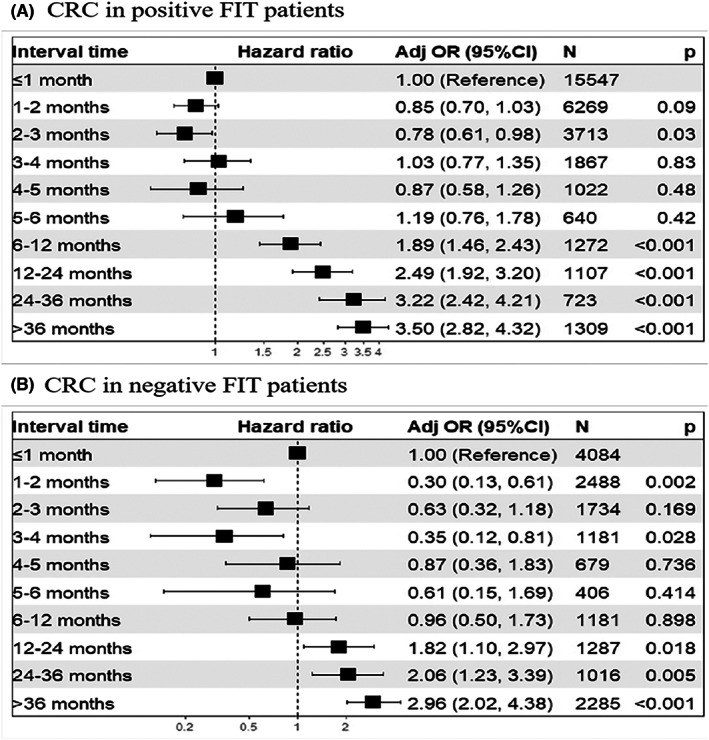
Results: Among the high-risk population without a history of CRC or polyps, 49,810 underwent HRFQ, FIT, and colonoscopy, and a time interval of fewer than 6 months was found for 79.56% of patients (n = 39,630). People with positive FIT were more likely to undergo colonoscopy within 6 months, and detection rates of CRC and/or advanced adenoma were positively related to time intervals. Similar results were found in people with a negative FIT but positive HRFQ. A time interval longer than 6 months was a significant predictor of CRC detection in high-risk populations.
Conclusion: For high-risk people identified by CRC screening, especially those with a positive FIT, a time interval of 6 months was associated with an increased probability of CRC detection. Our findings emphasize that populations at high risk should undergo colonoscopy at least within 6 months.
Keywords: cancer prevention; colonoscopy; colorectal cancer; colorectal cancer screening.
© 2023 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
The authors disclose no conflicts.
Figures
Comment in
-
Reply: Request for clarification on symptom assessment methodology in high-risk population colonoscopy study.Cancer Med. 2023 Jul;12(14):15629-15631. doi: 10.1002/cam4.6164. Epub 2023 Jun 2. Cancer Med. 2023. PMID: 37264753 Free PMC article. No abstract available.
-
Re: Postponing colonoscopy for 6 months in high-risk population increases colorectal cancer detection in China.Cancer Med. 2023 Jul;12(14):15628. doi: 10.1002/cam4.6227. Cancer Med. 2023. PMID: 37566104 Free PMC article. No abstract available.
Similar articles
-
[Efficacy comparison among high risk factors questionnaire and Asia-Pacific colorectal screening score and their combinations with fecal immunochemical test in screening advanced colorectal tumor].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Jul 25;25(7):612-620. doi: 10.3760/cma.j.cn441530-20211127-00478. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35844124 Chinese.
-
Factors associated with adherence to colonoscopy among individuals who were positive in the preliminary screening for colorectal neoplasms.Cancer Med. 2022 Nov;11(22):4321-4331. doi: 10.1002/cam4.4730. Epub 2022 Apr 20. Cancer Med. 2022. PMID: 35441812 Free PMC article.
-
Combining FITs and HRFQ with colonoscopy improve the cost-effectiveness of a 9-year mass colorectal cancer screening program.ESMO Open. 2024 Sep;9(9):103676. doi: 10.1016/j.esmoop.2024.103676. Epub 2024 Aug 20. ESMO Open. 2024. PMID: 39168026 Free PMC article.
-
Colorectal Cancer Screening: Recommendations for Physicians and Patients from the U.S. Multi-Society Task Force on Colorectal Cancer.Am J Gastroenterol. 2017 Jul;112(7):1016-1030. doi: 10.1038/ajg.2017.174. Epub 2017 Jun 6. Am J Gastroenterol. 2017. PMID: 28555630 Review.
-
Adenoma detection rate in colonoscopy: how can it be improved?Expert Rev Gastroenterol Hepatol. 2023 Jul-Dec;17(11):1089-1099. doi: 10.1080/17474124.2023.2273990. Epub 2023 Nov 23. Expert Rev Gastroenterol Hepatol. 2023. PMID: 37869781 Review.
Cited by
-
Re: Postponing colonoscopy for 6 months in high-risk population increases colorectal cancer detection in China.Cancer Med. 2023 Jul;12(14):15628. doi: 10.1002/cam4.6227. Cancer Med. 2023. PMID: 37566104 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
