

Imaging of Cartilage and Chondral Defects: An Overview
- PMID: 36836719
- PMCID: PMC9960762
- DOI: 10.3390/life13020363
Imaging of Cartilage and Chondral Defects: An Overview
Abstract
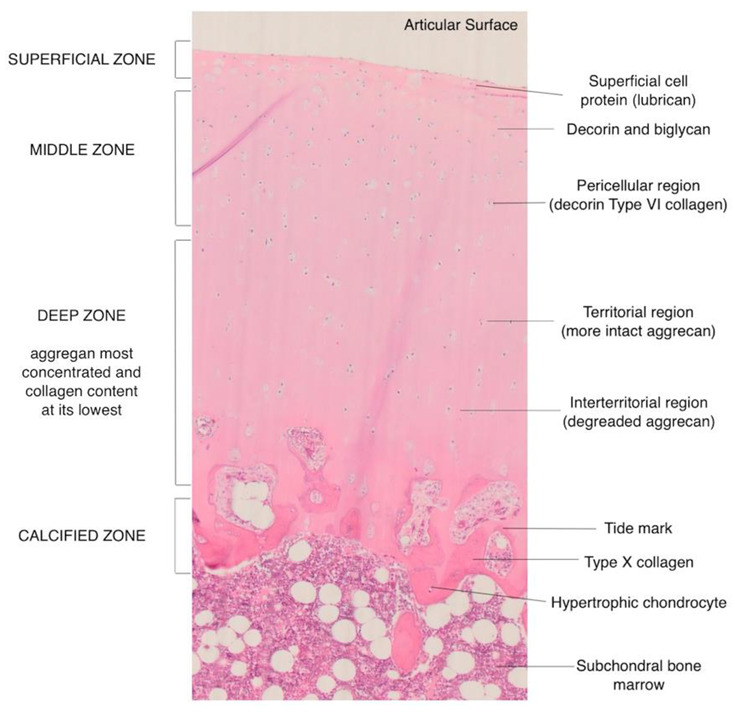
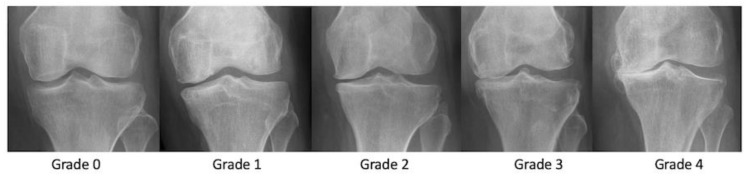
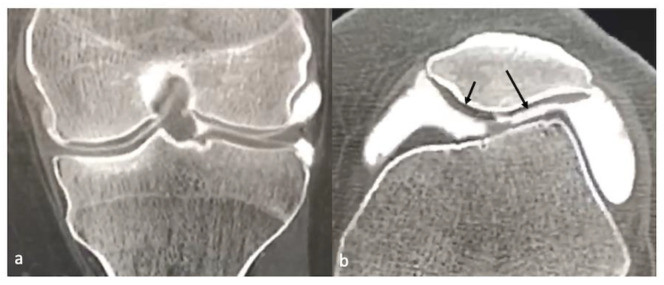
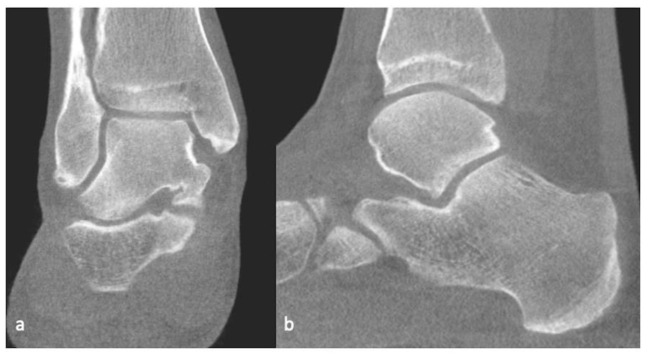
A healthy articular cartilage is paramount to joint function. Cartilage defects, whether acute or chronic, are a significant source of morbidity. This review summarizes various imaging modalities used for cartilage assessment. While radiographs are insensitive, they are still widely used to indirectly assess cartilage. Ultrasound has shown promise in the detection of cartilage defects, but its efficacy is limited in many joints due to inadequate visualization. CT arthrography has the potential to assess internal derangements of joints along with cartilage, especially in patients with contraindications to MRI. MRI remains the favored imaging modality to assess cartilage. The conventional imaging techniques are able to assess cartilage abnormalities when cartilage is already damaged. The newer imaging techniques are thus targeted at detecting biochemical and structural changes in cartilage before an actual visible irreversible loss. These include, but are not limited to, T2 and T2* mapping, dGEMRI, T1ρ imaging, gagCEST imaging, sodium MRI and integrated PET with MRI. A brief discussion of the advances in the surgical management of cartilage defects and post-operative imaging assessment is also included.
Keywords: MRI; cartilage imaging; chondral defects; osteoarthritis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




Similar articles
-
Advanced Imaging in Femoroacetabular Impingement: Current State and Future Prospects.Front Surg. 2015 Jul 24;2:34. doi: 10.3389/fsurg.2015.00034. eCollection 2015. Front Surg. 2015. PMID: 26258129 Free PMC article. Review.
-
Modern Cartilage Imaging of the Ankle.Rofo. 2017 Oct;189(10):945-956. doi: 10.1055/s-0043-110861. Epub 2017 Jul 11. Rofo. 2017. PMID: 28697530 Review. English.
-
Comparison between magnetic resonance imaging, computed tomography, and arthrography to identify artificially induced cartilage defects of the equine carpal joints.Vet Radiol Ultrasound. 2018 May;59(3):312-325. doi: 10.1111/vru.12598. Epub 2018 Feb 18. Vet Radiol Ultrasound. 2018. PMID: 29455473
-
Advances in magnetic resonance imaging of articular cartilage.J Am Acad Orthop Surg. 2011 Jul;19(7):420-9. doi: 10.5435/00124635-201107000-00005. J Am Acad Orthop Surg. 2011. PMID: 21724921 Review.
-
Cartilage T1ρ and T2 Relaxation Times in Patients With Mild-to-Moderate Radiographic Hip Osteoarthritis.Arthritis Rheumatol. 2015 Jun;67(6):1548-56. doi: 10.1002/art.39074. Arthritis Rheumatol. 2015. PMID: 25779656 Free PMC article.
Cited by
-
Quantitative and Compositional MRI of the Articular Cartilage: A Narrative Review.Tomography. 2024 Jun 24;10(7):949-969. doi: 10.3390/tomography10070072. Tomography. 2024. PMID: 39058044 Free PMC article. Review.
-
[Research progress in Oxford unicompartmental knee arthroplasty for partial thickness cartilage loss in medial compartment of knee joint].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024 Sep 15;38(9):1138-1142. doi: 10.7507/1002-1892.202403091. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2024. PMID: 39300891 Free PMC article. Review. Chinese.
-
MRI Features That Contribute to Decision-Making for Treatment of Capitellar OCD Lesions: An Expert Consensus Using the Delphi Method.Orthop J Sports Med. 2024 Jun 6;12(6):23259671241252813. doi: 10.1177/23259671241252813. eCollection 2024 Jun. Orthop J Sports Med. 2024. PMID: 38845610 Free PMC article.
-
A New Approach to Postoperative Rehabilitation following Mosaicplasty and Bone Marrow Aspiration Concentrate (BMAC) Augmentation.Biomedicines. 2024 May 24;12(6):1164. doi: 10.3390/biomedicines12061164. Biomedicines. 2024. PMID: 38927371 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
