

Airway remodeling heterogeneity in asthma and its relationship to disease outcomes
- PMID: 36744026
- PMCID: PMC9892557
- DOI: 10.3389/fphys.2023.1113100
Airway remodeling heterogeneity in asthma and its relationship to disease outcomes
Abstract
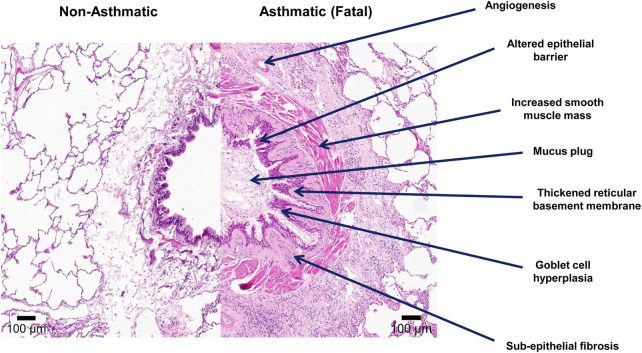
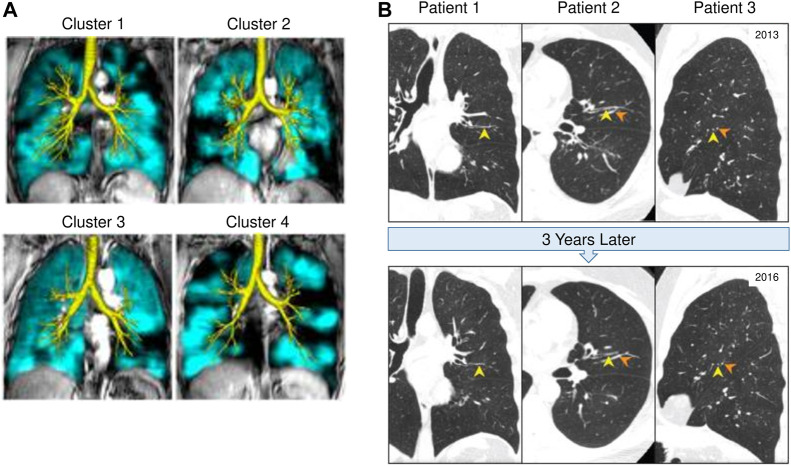
Asthma affects an estimated 262 million people worldwide and caused over 461,000 deaths in 2019. The disease is characterized by chronic airway inflammation, reversible bronchoconstriction, and airway remodeling. Longitudinal studies have shown that current treatments for asthma (inhaled bronchodilators and corticosteroids) can reduce the frequency of exacerbations, but do not modify disease outcomes over time. Further, longitudinal studies in children to adulthood have shown that these treatments do not improve asthma severity or fixed airflow obstruction over time. In asthma, fixed airflow obstruction is caused by remodeling of the airway wall, but such airway remodeling also significantly contributes to airway closure during bronchoconstriction in acute asthmatic episodes. The goal of the current review is to understand what is known about the heterogeneity of airway remodeling in asthma and how this contributes to the disease process. We provide an overview of the existing knowledge on airway remodeling features observed in asthma, including loss of epithelial integrity, mucous cell metaplasia, extracellular matrix remodeling in both the airways and vessels, angiogenesis, and increased smooth muscle mass. While such studies have provided extensive knowledge on different aspects of airway remodeling, they have relied on biopsy sampling or pathological assessment of lungs from fatal asthma patients, which have limitations for understanding airway heterogeneity and the entire asthma syndrome. To further understand the heterogeneity of airway remodeling in asthma, we highlight the potential of in vivo imaging tools such as computed tomography and magnetic resonance imaging. Such volumetric imaging tools provide the opportunity to assess the heterogeneity of airway remodeling within the whole lung and have led to the novel identification of heterogenous gas trapping and mucus plugging as important predictors of patient outcomes. Lastly, we summarize the current knowledge of modification of airway remodeling with available asthma therapeutics to highlight the need for future studies that use in vivo imaging tools to assess airway remodeling outcomes.
Keywords: airway heterogeneity; airway remodeling; asthma; asthma therapeutics; computed tomgraphy (CT); magnetic resonance imaging (MRI); mucus plug.
Copyright © 2023 Hsieh, Assadinia and Hackett.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Pathobiology of Airway Remodeling in Asthma: The Emerging Role of Integrins.J Asthma Allergy. 2022 May 11;15:595-610. doi: 10.2147/JAA.S267222. eCollection 2022. J Asthma Allergy. 2022. PMID: 35592385 Free PMC article. Review.
-
Imaging Regional Airway Involvement of Asthma: Heterogeneity in Ventilation, Mucus Plugs and Remodeling.Adv Exp Med Biol. 2023;1426:163-184. doi: 10.1007/978-3-031-32259-4_8. Adv Exp Med Biol. 2023. PMID: 37464121
-
Bidirectional interaction of airway epithelial remodeling and inflammation in asthma.Clin Sci (Lond). 2020 May 15;134(9):1063-1079. doi: 10.1042/CS20191309. Clin Sci (Lond). 2020. PMID: 32369100 Review.
-
Clinical assessment of airway remodeling in asthma: utility of computed tomography.Clin Rev Allergy Immunol. 2004 Aug;27(1):45-58. doi: 10.1385/CRIAI:27:1:045. Clin Rev Allergy Immunol. 2004. PMID: 15347850 Review.
-
Airway remodeling in asthma.Allergol Int. 2007 Dec;56(4):341-8. doi: 10.2332/allergolint.R-07-153. Epub 2007 Nov 1. Allergol Int. 2007. PMID: 17965577 Review.
Cited by
-
Targeting inflammation or remodeling in asthma? Is there a right way?Front Med (Lausanne). 2023 Nov 23;10:1241920. doi: 10.3389/fmed.2023.1241920. eCollection 2023. Front Med (Lausanne). 2023. PMID: 38076243 Free PMC article. No abstract available.
-
Rhinovirus induces airway remodeling: what are the physiological consequences?Respir Res. 2023 Sep 29;24(1):238. doi: 10.1186/s12931-023-02529-9. Respir Res. 2023. PMID: 37773065 Free PMC article. Review.
-
Airway remodelling in asthma and the epithelium: on the edge of a new era.Eur Respir J. 2024 Apr 18;63(4):2301619. doi: 10.1183/13993003.01619-2023. Print 2024 Apr. Eur Respir J. 2024. PMID: 38609094 Free PMC article. Review.
-
Research trends on airway remodeling: A bibliometrics analysis.Heliyon. 2024 Jan 20;10(3):e24824. doi: 10.1016/j.heliyon.2024.e24824. eCollection 2024 Feb 15. Heliyon. 2024. PMID: 38333835 Free PMC article.
-
Effects of Panax species and their bioactive components on allergic airway diseases.J Ginseng Res. 2024 Jul;48(4):354-365. doi: 10.1016/j.jgr.2024.04.003. Epub 2024 Apr 21. J Ginseng Res. 2024. PMID: 39036733 Free PMC article. Review.
References
-
- Aliyali M., Amiri A. P., Sharifpoor A., Zalli F. (2010). Effects of N-acetylcysteine on asthma exacerbation. Iran. J. Allergy Asthma Immunol. 9, 103–109. Published online. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources