

Intestinal Barrier Function in the Pathogenesis of Nonalcoholic Fatty Liver Disease
- PMID: 36643028
- PMCID: PMC9817057
- DOI: 10.14218/JCTH.2022.00089
Intestinal Barrier Function in the Pathogenesis of Nonalcoholic Fatty Liver Disease
Abstract
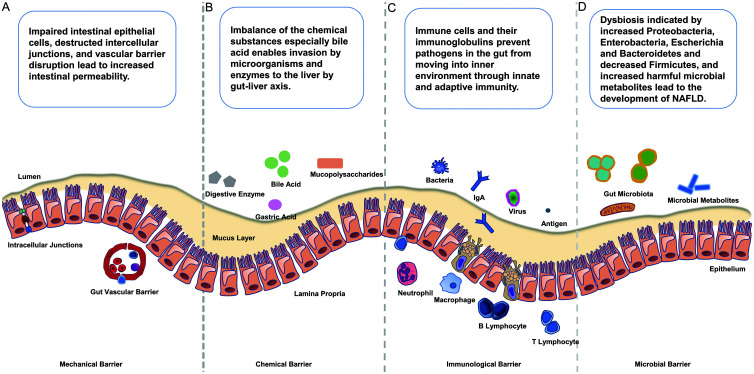
Nonalcoholic fatty liver disease (NAFLD) is the most common chronic liver disease worldwide. The mechanisms involved in NAFLD onset are complicated and multifactorial. Recent literature has indicated that altered intestinal barrier function is related to the occurrence and progression of liver disease. The intestinal barrier is important for absorbing nutrients and electrolytes and for defending against toxins and antigens in the enteric environment. Major mechanisms by which the intestinal barrier influences the development of NAFLD involve the altered epithelial layer, decreased intracellular junction integrity, and increased intestinal barrier permeability. Increased intestinal permeability leads to luminal dysbiosis and allows the translocation of pathogenic bacteria and metabolites into the liver, inducing inflammation, immune response, and hepatocyte injury in NAFLD. Although research has been directed to NAFLD in recent decades, the pathophysiological changes in NAFLD initiation and progression are still not completely understood, and the therapeutic targets remain limited. A deeper understanding on the correlation between NAFLD pathogenesis and intestinal barrier regulation must be attained. Therefore, in this review, the components of the intestinal barrier and their respective functions and disruptions during the progression of NAFLD are discussed.
Keywords: Gut-liver axis; Intestinal barrier; Intestinal barrier permeability; Nonalcoholic fatty liver disease.
© 2023 Authors.
Conflict of interest statement
The authors have no conflict of interests related to this publication.
Figures
Similar articles
-
The Role of Leaky Gut in Nonalcoholic Fatty Liver Disease: A Novel Therapeutic Target.Int J Mol Sci. 2021 Jul 29;22(15):8161. doi: 10.3390/ijms22158161. Int J Mol Sci. 2021. PMID: 34360923 Free PMC article. Review.
-
The Role of Gut-Liver Axis in Gut Microbiome Dysbiosis Associated NAFLD and NAFLD-HCC.Biomedicines. 2022 Feb 23;10(3):524. doi: 10.3390/biomedicines10030524. Biomedicines. 2022. PMID: 35327326 Free PMC article. Review.
-
Intestinal permeability in human nonalcoholic fatty liver disease: A systematic review and meta-analysis.Liver Int. 2020 Dec;40(12):2906-2916. doi: 10.1111/liv.14696. Epub 2020 Oct 21. Liver Int. 2020. PMID: 33037768 Free PMC article. Review.
-
Gut dysbiosis in nonalcoholic fatty liver disease: pathogenesis, diagnosis, and therapeutic implications.Front Cell Infect Microbiol. 2022 Nov 8;12:997018. doi: 10.3389/fcimb.2022.997018. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 36425787 Free PMC article. Review.
-
Contribution of gut microbiota to nonalcoholic fatty liver disease: Pathways of mechanisms.Clin Nutr ESPEN. 2021 Aug;44:61-68. doi: 10.1016/j.clnesp.2021.05.012. Epub 2021 May 25. Clin Nutr ESPEN. 2021. PMID: 34330514 Review.
Cited by
-
Probiotics for inflammatory bowel disease: Is there sufficient evidence?Open Life Sci. 2024 Apr 5;19(1):20220821. doi: 10.1515/biol-2022-0821. eCollection 2024. Open Life Sci. 2024. PMID: 38585636 Free PMC article. Review.
-
Multi-system diseases and death trajectory of metabolic dysfunction-associated fatty liver disease: findings from the UK Biobank.BMC Med. 2023 Oct 20;21(1):398. doi: 10.1186/s12916-023-03080-6. BMC Med. 2023. PMID: 37864216 Free PMC article.
-
Intestinal changes in permeability, tight junction and mucin synthesis in a mouse model of Alzheimer's disease.Int J Mol Med. 2023 Dec;52(6):113. doi: 10.3892/ijmm.2023.5316. Epub 2023 Oct 13. Int J Mol Med. 2023. PMID: 37830152 Free PMC article.
-
Role of gut-liver axis and glucagon-like peptide-1 receptor agonists in the treatment of metabolic dysfunction-associated fatty liver disease.World J Gastroenterol. 2024 Jun 21;30(23):2964-2980. doi: 10.3748/wjg.v30.i23.2964. World J Gastroenterol. 2024. PMID: 38946874 Free PMC article. Review.
-
Roles of gut microbes in metabolic-associated fatty liver disease.Tzu Chi Med J. 2023 Jul 11;35(4):279-289. doi: 10.4103/tcmj.tcmj_86_23. eCollection 2023 Oct-Dec. Tzu Chi Med J. 2023. PMID: 38035063 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources